
Predictive values of IL-33, EMPs and TF for heart failure in patients with acute myocardial infarction
-
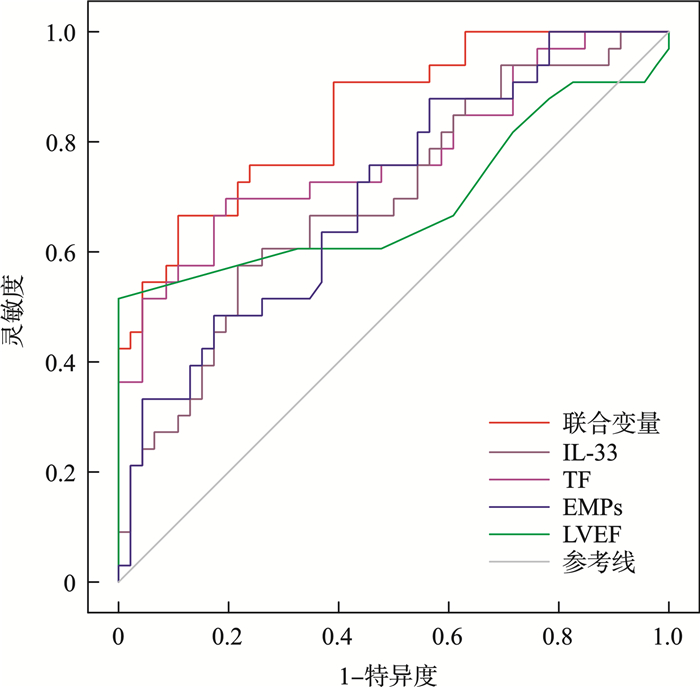
摘要: 目的 探讨IL-33、内皮细胞微粒(endothelial cell microparticles,EMPs)及其表面组织因子(tissue factor,TF)在预测急性心肌梗死(acute myocardial infarction,AMI)患者院内早期心力衰竭方面的价值。方法 本研究纳入2021年1月—2022年12月在我院确诊为AMI的79例患者,根据入院后24 h内是否出现心力衰竭(heart failure,HF)分为两组:AMI组(46例)和AMI合并心力衰竭组(AMI-HF组,33例)。另选择同期住院的77例稳定型冠心病患者(CAD组)作为对照组。通过流式细胞术检测EMPs水平、ELISA法检测IL-33和EMPs表面TF的表达水平。结果 AMI-HF组的IL-33、EMPs、EMPs表面TF水平显著高于AMI组(P<0.001),也高于CAD组,差异有统计学意义(P<0.001);回归分析表明,IL-33、EMPs、TF为AMI患者院内早期发生心力衰竭的独立危险因素(P<0.05);从ROC曲线分析显示,TF的曲线下面积为0.772(95%CI:0.662~0.882,P<0.001),IL-33的曲线下面积为0.695(95%CI:0.577~0.813,P=0.003),EMPs的曲线下面积为0.703(95%CI:0.587~0.812,P=0.002),而联合变量的曲线下面积则为0.847(95%CI:0.764~0.932,P<0.001)。ROC曲线显示,IL-33、EMPs和TF联合预测在AMI患者院内发生心力衰竭时,其AUC值超过了各个指标单独预测的AUC值。结论 IL-33、TF、EMPs与AMI患者在院内发生早期心力衰竭有关,并且对AMI患者在院内发生早期心力衰竭具有一定的预测作用,而且三者的联合预测效果较常用心力衰竭检测指标更为显著。
-
关键词:
- 急性心肌梗死后心力衰竭 /
- 内皮细胞微粒 /
- IL-33 /
- 组织因子
Abstract: Objective To evaluate the predictive value of IL-33, endothelial cell microparticles (EMPs), tissue factor (TF) in relation to the early development of heart failure during hospitalization in patients with acute myocardial infarction (AMI).Methods A total of AMI group (n=79) divided into AMI group (n=46) and AMI-HF group (n=33), A control group of 77 patients with stable patients with coronary heart disease (CAD group) visited the Department of Cardiology. Blood samples were obtained from all patients, with EMP levels analyzed through flow cytometry, while IL-33 and TF concentrations were measured using ELISA techniques.Results The levels of IL-33, EMPs, and TF in the AMI-HF group were significantly elevated compared to those in the AMI group (P < 0.0001) and also surpassed the levels in the CAD group (P < 0.0001). Univariate and multivariate logistic regression analyses indicated that IL-33, EMPs, and TF serve as independent risk factors for the early development of heart failure in acute myocardial infarction patients (P < 0.05). ROC curve analysis revealed that TF (area under the curve=0.772, 95%CI: 0.662-0.882, P < 0.001), IL-33(area under the curve=0.695, 95%CI: 0.577-0.813, P=0.003), EMPs (area under the curve=0.703, 95%CI: 0.587-0.812, P=0.002), and covariates (area under the curve=0.847, 95%CI: 0.764-0.932, P < 0.001).Conclusion IL-33, TF, and EMPs are linked to early heart failure in hospitalized AMI patients and demonstrate a notable predictive capability for early heart failure in this population. Furthermore, the combined predictive effect of these three biomarkers is more pronounced than that of standard heart failure diagnostic markers. -

-
表 1 各组患者一般临床资料比较
项目 CAD组(76例) AMI组(46例) AMI-HF(33例) F/Z/χ2 P 年龄/岁 60(56.00,67.50) 58(59.00,67.00) 57(47.75,67.75) 1.580 0.209 男/例(%) 54(71.1) 37(80.4) 23(69.7) 1.616 0.446 BMI/(kg/m2) 25.68(24.08,27.00) 27.10(23.98,29.73) 25.26(22.98,29.39) 3.336 0.189 糖尿病史/例(%) 23(30.3) 13(31.0) 8(26.7) 14.942 0.005 高血压病史/例(%) 41(53.9) 20(48.8) 13(43.3) 15.131 0.004 吸烟史/例(%) 11(14.5) 29(63.0) 19(57.6) 47.380 <0.001 阿司匹林/例(%) 64(84.2) 45(97.8) 28(84.8) 0.058 5.687 氯吡格雷/例(%) 60(78.9) 43(93.5) 26(78.8) 0.085 4.926 β受体阻滞剂/例(%) 69(90.8) 42(91.3) 30(90.9) 0.009 0.995 ACEI/ARB/例(%) 32(42.1) 17(37.0) 18(54.5) 2.499 0.287 他汀类/例(%) 69(90.8) 46(100.0) 26(78.8) 10.529 0.005 收缩压/mmHg 133(118.25,151.50) 131(115.00,148.00) 124(111.25,147.00) 3.641 0.162 舒张压/mmHg 80.0(74.00,88.75) 79.0(70.00,90.00) 74.5(66.00,86.25) 2.836 0.242 Gensini评分/分 20(7.75,31.75) 14(6.00,25.00) 18(10.00,32.00) 1.210 0.546 WBC/(×109/L) 6.22(5.03,8.35) 9.88(6.18,12.19) 9.87(8.08,11.98) 45.719 <0.001 RBC/(×109/L) 4.72(4.41,5.14) 4.78(4.37,5.03) 4.62(4.28,4.91) 1.326 0.515 PLT/(×109/L) 235.00(92.50,276.00) 216.00(88.00,298.00) 237.50(96.50,301.25) 1.355 0.508 CRP/(mg/L) 2.65(1.91,4.38) 3.29(1.26,8.10) 3.49(2.48,10.49) 4.234 0.120 TC/(mmol/L) 4.11±1.20 4.27±1.84 4.45±1.00 0.698 0.499 TG/(mmol/L) 1.41(0.97,1.97) 1.39(0.94,2.06) 1.29(0.99,1.91) 0.261 0.878 LDL-C/(mmol/L) 2.27±0.90 2.56±1.19 2.95±0.92 5.349 0.006 HDL-C/(mmol/L) 0.87(0.78,0.99) 0.97(0.76,1.09) 1.06(0.85,1.21) 6.260 0.044 GLU/(mmol/L) 5.56(4.64,6.25) 5.94(5.08,7.93) 7.32(5.49,9.28) 12.141 0.002 cTnT/(ng/mL) 0.10(0.01,0.02) 0.42(0.15,1.51) 0.36(0.05,1.95) 70.424 <0.001 CK-MB/(ng/mL) 10.14(0.97,16.11) 26(2.40,100.00) 33.75(3.22,153.20) 20.270 <0.001 BNP/(pg/mL) 89.60(54.10,177.03) 662.50(393.80,844.68) 903.90(567.90,970.50) 122.650 <0.001 LVEF/% 52(50,56) 52(50.56) 47(45,54) 13.236 <0.001 注:1 mmHg=0.133 kPa。PLT,血小板计数;CRP,C反应蛋白;TC,总胆固醇;TG,甘油三酯。  下载: 导出CSV
下载: 导出CSV
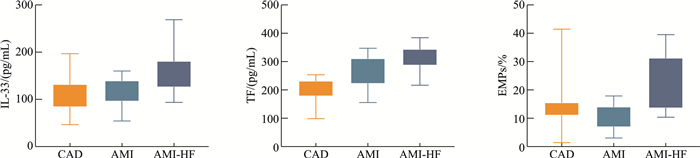
表 2 各组患者IL-33、EMPs、TF比较
X±S 变量 CAD组(76例) AMI组(46例) AMI-HF(33例) F P IL-33/(pg/mL) 102.91±30.28 115.15±41.93 145.78±41.07 15.928 <0.001 EMPs/% 10.14±6.03 13.43±4.95 18.07±6.83 21.010 <0.001 TF/(pg/mL) 200.08±41.02 290.75±41.9 339.2±51.31 136.914 <0.001
下载: 导出CSV
表 3 单因素logistic回归分析AMI后心力衰竭患者危险因素
变量 OR 95%CI P 年龄 0.991 0.954~1.030 0.654 性别 1.787 0.632~5.058 0.274 BMI 0.928 0.824~1.045 0.218 高血压 1.553 0.765~3.151 0.223 糖尿病 1.133 0.692~1.133 0.692 吸烟 0.796 0.319~1.984 0.624 阿司匹林 0.124 0.014~1.121 0.063 氯吡格雷 0.259 0.062~1.091 0.066 β受体阻滞剂 0.952 0.198~4.571 0.951 ACEI/ARB 2.047 0.824~5.085 0.123 TC 1.074 0.800~1.443 0.633 TG 0.885 0.677~1.155 0.368 LDL-C 1.409 0.913~2.176 0.122 HDL-C 1.678 0.496-5.672 0.405 GLU 1.001 0.999~1.002 0.455 cTnT 0.885 0.637~1.230 0.467 CK-MB 1.002 0.998~1.006 0.370 BNP 0.112 0.999~1.003 0.112 LVEF 0.856 0.768~0.955 0.005 IL-33 1.018 1.006~1.031 0.004 EMPs 1.160 1.049~1.284 0.004 TF 1.027 1.012~1.042 <0.001
下载: 导出CSV
表 4 多因素logistic回归分析AMI后心力衰竭患者危险因素
变量 OR 95%CI P LVEF 0.801 0.695~0.924 0.002 IL-33 1.017 1.002~1.032 <0.001 TF 1.005 1.008~1.040 0.022 EMPs 1.149 1.020~1.295 0.027
下载: 导出CSV
-
[1] Mensah GA, Fuster V, Murray CJL, et al. Global burden of cardiovascular diseases and risks, 1990-2022[J]. J Am Coll Cardiol, 2023, 82(25): 2350-2473. doi: 10.1016/j.jacc.2023.11.007
[2] Avolio E, Campagnolo P, Katare R, et al. The role of cardiac pericytes in health and disease: therapeutic targets for myocardial infarction[J]. Nat Rev Cardiol, 2024, 21(2): 106-118. doi: 10.1038/s41569-023-00913-y
[3] Klingenberg R, Aghlmandi S, Räber L, et al. Improved risk stratification of patients with acute coronary syndromes using a combination of hsTnT, NT-proBNP and hsCRP with the GRACE score[J]. Eur Heart J Acute Cardiovasc Care, 2018, 7(2): 129-138. doi: 10.1177/2048872616684678
[4] Chen WY, Tsai TH, Yang JL, et al. Therapeutic strategies for targeting IL-33/ST2 signalling for the treatment of inflammatory diseases[J]. Cell Physiol Biochem, 2018, 49(1): 349-358. doi: 10.1159/000492885
[5] Cayrol C, Girard JP. Interleukin-33(IL-33): a critical review of its biology and the mechanisms involved in its release as a potent extracellular cytokine[J]. Cytokine, 2022, 156: 155891. doi: 10.1016/j.cyto.2022.155891
[6] Witkowska A, Staciwa M, Duraj I, et al. Interleukin-33/sST2: dynamic assessment in patients with acute coronary syndrome[J]. Adv Med Sci, 2023, 68(2): 195-201. doi: 10.1016/j.advms.2023.05.001
[7] Mattera V, Occhiuzzi F, Correale J, et al. Remyelinating effect driven by transferrin-loaded extracellular vesicles[J]. Glia, 2024, 72(2): 338-361. doi: 10.1002/glia.24478
[8] Alexandru N, Andrei E, Safciuc F, et al. Intravenous administration of allogenic cell-derived microvesicles of healthy origins defend against atherosclerotic cardiovascular disease development by a direct action on endothelial progenitor cells[J]. Cells, 2020, 9(2): 423. doi: 10.3390/cells9020423
[9] Kobayashi H, Matsubara S, Imanaka S. The role of tissue factor pathway inhibitor 2 in the coagulation and fibrinolysis system[J]. J Obstet Gynaecol Res, 2023, 49(7): 1677-1683. doi: 10.1111/jog.15660
[10] Chiva-Blanch G, Laake K, Myhre P, et al. Platelet-, monocyte-derived and tissue factor-carrying circulating microparticles are related to acute myocardial infarction severity[J]. PLoS One, 2017, 12(2): e0172558. doi: 10.1371/journal.pone.0172558
[11] Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction(2018)[J]. J Am Coll Cardiol, 2018, 72(18): 2231-2264.
[12] 张健, 张宇辉, 周蕾. 国家心力衰竭指南2023(精简版)[J]. 中国循环杂志, 2023, 38(12): 1207-1238.
[13] Zhang Z, Chen F, Wan JJ, et al. Potential traditional Chinese medicines with anti-inflammation in the prevention of heart failure following myocardial infarction[J]. Chin Med, 2023, 18(1): 28.
[14] Bahit MC, Kochar A, Granger CB. Post-myocardial infarction heart failure[J]. JACC Heart Fail, 2018, 6(3): 179-186.
[15] He YF, Wu Q. The effect of extracellular vesicles on thrombosis[J]. J Cardiovasc Transl Res, 2023, 16(3): 682-697. doi: 10.1007/s12265-022-10342-w
[16] 吐尔孙阿依·依斯米提拉, 阿里米江·阿布里米提, 麦合甫热提·乌甫尔, 等. 动脉粥样硬化中的IL-33/ST2通路: IL-33悖论[J]. 中华全科医学, 2023, 21(1): 19-23.
[17] Frantz S, Hundertmark MJ, Schulz-Menger J, et al. Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies[J]. Eur Heart J, 2022, 43(27): 2549-2561. doi: 10.1093/eurheartj/ehac223
[18] Peng XY, Du J, Wang Y. Metabolic signatures in post-myocardial infarction heart failure, including insights into prediction, intervention, and prognosis[J]. Biomed Pharmacother, 2024, 170: 116079.
[19] Elia E, Montecucco F, Portincasa P, et al. Update on pathological platelet activation in coronary thrombosis[J]. J Cell Physiol, 2019, 234(3): 2121-2133. doi: 10.1002/jcp.27575
[20] Yan XL, Guo YQ, Li L, et al. The sST2 level is an independent influencing factor associated with atrial fibrillation in heart failure patients: a case-control study[J]. J Thorac Dis, 2022, 14(5): 1578-1587.
[21] Lugrin J, Parapanov R, Milano G, et al. The systemic deletion of interleukin-1α reduces myocardial inflammation and attenuates ventricular remodeling in murine myocardial infarction[J]. Sci Rep, 2023, 13(1): 4006.
[22] 袁玉娟, 李吉斌, 李昊, 等. 急性心肌梗死与冠状动脉血内皮细胞源微粒、组织因子和白细胞介素-33的相关性研究[J]. 临床心血管病杂志, 2021, 37(4): 328-332.
[23] Ye YY, Chang FY, Xu YC. IL-33 in atherosclerosis: an insufficiently explored and controversial research area[J]. Cardiovasc Drugs Ther, 2024, 38(3): 419-420.
-
计量
- 文章访问数: 111
- 施引文献: 0