
Study on the characteristics of sublingual microcirculation in sepsis-associated coagulopathy and the correlation between inflammation-coagulation-microcirculation indicators and short-term prognosis
-
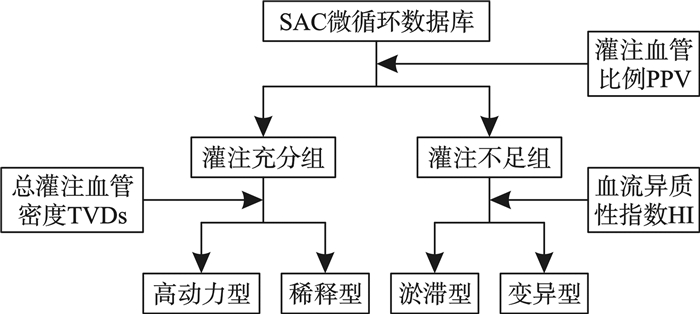
摘要: 目的 探讨脓毒症相关凝血病患者舌下微循环特征及凝血、炎症及舌下微循环指标对其短期预后的影响。方法 采用回顾性队列研究,纳入2023年12月1日—2024年6月30日在四川大学华西医院急诊科就诊且符合脓毒症相关凝血病诊断的患者,收集患者入院后48 h内酸碱度、血乳酸水平、平均动脉压、白细胞计数、血小板计数、降钙素原水平、活化部分凝血活酶时间(activated partial thromboplastin time,APTT)、血浆凝血酶原时间、国际正常化比值、纤维蛋白原、D-二聚体及舌下微循环指标。并根据总小血管密度(total vessels density small,TVDs)、灌注小血管密度(perfused vessels density small,PVDs)、灌注血管比例(proportion of perfused vessels,PPV)、微血管流动指数、异质性指数,将总体分为:淤滞型、稀释型、变异型和高动力型舌下微循环障碍,随访患者28 d生存情况。采用logistic回归模型分析影响脓毒症相关凝血病患者28 d病死率的炎症-凝血-微循环危险因素。结果 共纳入101例脓毒症相关凝血病患者,其中淤滞型8例(7.9%),稀释型15例(14.9%),变异型31例(30.7%),高动力型47例(46.5%)。单因素分析发现,各型间的TVDs、PVDs、PPV、28 d生存率差异有统计学意义。其中,淤滞型患者的PPV及28 d生存率均显著低于其他组,同时稀释型患者的总(灌注)血管密度显著低于其他组, 差异有统计学意义(P < 0.05)。二元logistic回归分析显示,APTT(OR=0.136,95%CI:1.045~1.257,P=0.004)、D-二聚体(OR=0.083,95%CI:1.023~1.154,P=0.007)、降钙素原(OR=0.089,95%CI:1.037~1.153,P=0.001)、灌注血管密度(OR=-5.54,95%CI:0.01~0.73,P=0.038)为影响脓毒症28 d病死率的独立危险因素。结论 脓毒症相关凝血病患者呈现特异性微循环障碍,其中淤滞型占比较高且预后差,炎症、凝血及微循环指标与短期预后独立相关。Abstract: Objective To explore the characteristics of sublingual microcirculation and the impact of coagulation, inflammation and sublingual microcirculation indicators on short-term prognosis in patients with sepsis-associated coagulopathy.Methods A retrospective cohort study was conducted, including patients diagnosed with sepsis-associated coagulopathy who visited the emergency department of West China Hospital, Sichuan University, between December 1, 2023 and June 30, 2024. Data collected within 48 hours of admission included pH, blood lactate levels, mean arterial pressure, white blood cell count, platelet count, procalcitonin levels, activated partial thromboplastin time(APTT), prothrombin time, international normalized ratio, fibrinogen, D-dimer and sublingual microcirculation parameters. According to the total small vessel density(TVDs), perfused small vessel density(PVDs), perfused vessel ratio(PPV), microvascular flow index(MFI) and heterogeneity index, patients were divided into four types of sublingual microcirculatory disorders: stagnation type, dilution type, variation type and hyperdynamic type. The 28-day survival status was followed up. Logistic regression models were used to analyze the inflammatory-coagulation-microcirculation risk factors affecting 28-day mortality in patients with sepsis-associated coagulopathy.Results A total of 101 patients with sepsis-associated coagulopathy were included, among which 8 patients(7.9%) were classified as stagnation type, 15(14.9%) as dilution type, 31(30.7%) as variation type and 47(46.5%) as hyperdynamic type. Univariate analysis revealed statistically significant differences in TVDs, PVDs, PPV and 28-day survival rates among the groups. Specifically, the perfused vessel ratio and 28-day survival rate in the stagnation type were significantly lower than those in the other groups, while the total/perfused vessel density in the dilution type was significantly lower than in the other groups, the difference was statistically significant(P < 0.05). Binary logistic regression analysis showed that APTT(OR=0.136, 95%CI: 1.045-1.257, P=0.004), D-dimer(OR=0.083, 95%CI: 1.023-1.154, P=0.007), procalcitonin(OR=0.089, 95%CI: 1.037-1.153, P=0.001) and perfused vessel density(OR=-5.54, 95%CI: 0.01-0.73, P=0.038) were independent risk factors for 28-day mortality in patients with sepsis.Conclusion Sepsis-associated coagulopathy patients exhibit distinct sublingual microcirculatory disorders, with the stagnation type being more prevalent and associated with poor prognosis. Inflammation, coagulation and microcirculation indicators are independently related to short-term prognosis.
-
Key words:
- sepsis /
- coagulopathy /
- coagulation dysfunction /
- microcirculatory disorders /
- short-term prognosis
-

-
表 1 不同舌下微循环障碍类型SAC患者一般临床资料
M(P25,P75),X±S 一般资料 总体(101例) 淤滞型(8例) 稀释型(15例) 变异型(31例) 高动力型(47例) 性别/例 男 65 4 8 25 28 女 36 4 7 6 19 年龄/岁 60(23,87) 63(29,87) 70(32,85) 60(23,87) 59(30,87) 平均动脉压/mmHg 79±15 73±9 78±14 74±13 84±17 住院时间/d 14(1,68) 8(2,23) 22(2,36) 7(1,55) 16(2,68) 注:1 mmHg=0.133 kPa。  下载: 导出CSV
下载: 导出CSV
表 2 不同微循环类型SAC患者的短期预后
类型 生存组/例 死亡组/例 28 d生存率/% 淤滞型 1 7 12.5 稀释型 10 5 66.7 变异型 6 25 19.4 高动力型 44 3 93.6 总体 61 40 60.4
下载: 导出CSV
表 3 不同舌下微循环障碍类型SAC患者的临床指标
X±S 临床指标 总体(101例) 淤滞型(8例) 稀释型(15例) 变异型(31例) 高动力型(47例) 微循环指标 TVDs/(mm/mm2) 8.72±2.78 10.10(7.40,18.10) 5.90(3.10,7.90) 7.53±2.96 9.72±2.31 PVDs/(mm/mm2) 7.62±2.93 7.80(6.10,14.70) 5.30(2.50,6.90) 5.70±2.46 9.41±2.32 PPV/% 86.3±14.70 81.30(67.40,84.90) 93.60(59.20,100.00) 71.10±17.60 96.30±3.37 MFI 2.36±0.61 2.67(2.22,3.00) 2.63(2.11,3.00) 1.63±0.54 2.72±0.24 HI 0.81±0.73 0.58(0,0.90) 0.41(0,0.92) 1.58±0.50 0.33±0.24 凝血指标 PT/s 18.70±7.49 19.20(13.50,40.80) 17.40(12.70,38.40) 18.00(13.40,36.80) 16.90±7.40 APTT/s 41.60±16.10 43.90(33.40,99.90) 39.00(27.60,69.30) 41.90(29.30,112.00) 35.70±20.00 INR 1.63±0.70 1.66(1.20,3.72) 1.52(1.09,3.49) 1.55(1.13,3.31) 1.47±0.71 纤维蛋白原/(g/L) 4.06±2.19 4.17(1.59,8.36) 3.17(1.22,8.36) 4.31(0.64,7.83) 4.26±2.24 D-二聚体/(mg/FEU) 10.10±9.61 6.59(0.86,34.50) 8.82(0.93,38.00) 9.28(1.23,38.00) 9.19±9.86
下载: 导出CSV
表 4 SAC患者预后危险因素分析
指标 生存组(61例) 死亡组(40例) P 性别/例(%) 0.434 男 36(59.0) 29(72.5) 女 25(41.0) 11 (27.5) 年龄/年 60(30, 87) 61(23, 87) 0.307 住院时间/d 18(2, 68) 6(1, 25) 0.001 代谢及炎症指标 平均动脉压/mmHg 83.61±15.81 74.19±12.68 0.020 pH 7.44±0.08 7.39±0.12 0.779 乳酸/(mmol/L) 2.02±1.02 3.65±3.93 0.024 白细胞计数/(×109/L) 14.34±10.44 14.95±12.02 0.173 降钙素原/(ng/mL) 1.78(0.12,30.00) 12.03(0.37,100.00) 0.002 凝血指标 血小板计数/(×109/L) 157±148 137±111 0.435 凝血酶原时间/s 15.51±2.35 23.57±9.76 0.419 APTT/s 34.94±6.16 51.64±20.73 0.004 INR 1.34±0.21 2.08±0.92 0.669 纤维蛋白原/(g/L) 4.40±2.26 3.56±2.01 0.239 D-二聚体/(mg/FEU) 6.30(0.29,38.00) 9.82(1.74,38.00) 0.007 微循环指标 TVDs/(mm/mm2) 8.95±2.48 8.38±3.17 0.044 PVDs/(mm/mm2) 8.62±2.48 6.08±2.92 0.038 PPV/% 95.86±3.96 71.92±16.13 0.913 HI 0.46±0.43 1.33±0.78 0.511 MFI 2.61±0.39 1.97±0.67 0.276 注:INR为国际正常化比值。
下载: 导出CSV
-
[1] Singh B, Hanson AC, Alhurani R, et al. Trends in the incidence and outcomes of disseminated intravascular coagulation in critically ill patients(2004-2010) A population-based study[J]. Chest, 2013, 143(5): 1235-1242. doi: 10.1378/chest.12-2112
[2] Lyons PG, Micek ST, Hampton N, et al. Sepsis-associated coagulopathy severity predicts hospital mortality[J]. Crit Care Med, 2018, 46(5): 736-742. doi: 10.1097/CCM.0000000000002997
[3] Levi M, van der Poll T. Coagulation and sepsis[J]. Thromb Res, 2017, 149: 38-44. doi: 10.1016/j.thromres.2016.11.007
[4] Iba T, Levi M, Thachil J, et al. Disseminated intravascular coagulation: the past, present, and future considerations[J]. Semin Thromb Hemost, 2022, 48(8): 978-987. doi: 10.1055/s-0042-1756300
[5] Verdant CL, De Backer D, Bruhn A, et al. Evaluation of sublingual and gut mucosal microcirculation in sepsis: a quantitative analysis[J]. Crit Care Med, 2009, 37(11): 2875-2881. doi: 10.1097/CCM.0b013e3181b029c1
[6] De Backer D, Creteur J, Preiser JC, et al. Microvascular blood flow is altered in patients with sepsis[J]. Am J Respir Crit Care Med, 2002, 166(1): 98-104. doi: 10.1164/rccm.200109-016OC
[7] Trzeciak S, Dellinger RP, Parrillo JE, et al. Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival[J]. Ann Emerg Med, 2007, 49(1): 88-98. e2. doi: 10.1016/j.annemergmed.2006.08.021
[8] Fan SH, Pang MM, Si M, et al. Quantitative changes in platelet count in response to different pathogens: an analysis of patients with sepsis in both retrospective and prospective cohorts[J]. Ann Med, 2024, 56(1): 2405073. doi: 10.1080/07853890.2024.2405073
[9] Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock(sepsis-3)[J]. JAMA, 2016, 315(8): 801-810. doi: 10.1001/jama.2016.0287
[10] 宋景春, 丁仁彧, 吕奔, 等. 脓毒症性凝血病诊疗中国专家共识[J/OL]. 解放军医学杂志, 2024(2024-09-24).
https://kns.cnki.net/kcms/detail/11.1056.R.20240923.1715.002.html .[11] Ince C, Boerma EC, Cecconi M, et al. Second consensus on the assessment of sublingual microcirculation in critically ill patients: results from a task force of the European society of intensive care medicine[J]. Intensive Care Med, 2018, 44(3): 281-299. doi: 10.1007/s00134-018-5070-7
[12] 郑瑞强, 张艺芬, 荣子琪, 等. 《拯救脓毒症运动: 脓毒症与感染性休克治疗国际指南2021版》解读与展望[J]. 中华危重病急救医学, 2021, 33(10): 1159-1164.
[13] Duranteau J, De Backer D, Donadello K, et al. The future of intensive care: the study of the microcirculation will help to guide our therapies[J]. Crit Care, 2023, 27(1): 190. doi: 10.1186/s13054-023-04474-x
[14] Edul VS, Enrico C, Laviolle B, et al. Quantitative assessment of the microcirculation in healthy volunteers and in patients with septic shock[J]. Crit Care Med, 2012, 40(5): 1443-1448. doi: 10.1097/CCM.0b013e31823dae59
[15] Trzeciak S, McCoy JV, Phillip Dellinger R, et al. Early increases in microcirculatory perfusion during protocol-directed resuscitation are associated with reduced multi-organ failure at 24 h in patients with sepsis[J]. Intensive Care Med, 2008, 34(12): 2210-2217. doi: 10.1007/s00134-008-1193-6
[16] Sakr Y, Dubois MJ, De Backer D, et al. Persistent microcirculatory alterations are associated with organ failure and death in patients with septic shock[J]. Crit Care Med, 2004, 32(9): 1825-1831. doi: 10.1097/01.CCM.0000138558.16257.3F
[17] De Backer D, Donadello K, Sakr Y, et al. Microcirculatory alterations in patients with severe sepsis: impact of time of assessment and relationship with outcome[J]. Crit Care Med, 2013, 41(3): 791-799. doi: 10.1097/CCM.0b013e3182742e8b
[18] Levi M, Poll Tv. Coagulation in patients with severe sepsis[J]. Semin Thromb Hemost, 2015, 41(1): 9-15. doi: 10.1055/s-0034-1398376
[19] Levi M, van der Poll T. Inflammation and coagulation[J]. Crit Care Med, 2010, 38(2 suppl): S26-S34.
[20] Williams B, Zou L, Pittet JF, et al. Sepsis-induced coagulopathy: a comprehensive narrative review of pathophysiology, clinical presentation, diagnosis, and management strategies[J]. Anesth Analg, 2024, 138(4): 696-711.
[21] Semeraro N, Ammollo CT, Semeraro F, et al. Coagulopathy of acute sepsis[J]. Semin Thromb Hemost, 2015, 41(6): 650-658. doi: 10.1055/s-0035-1556730
[22] 张晓蕾, 李莉, 彭倩宜, 等. 感染性休克患者舌下微循环障碍分型及与预后的研究初探[J]. 中华内科杂志, 2021, 60(10): 898-903.
[23] Kim SM, Kim SI, Yu G, et al. Hypercoagulability in septic shock patients with thrombocytopenia[J]. J Intensive Care Med, 2022, 37(6): 721-727. doi: 10.1177/08850666211024188
[24] 周亚雄, 李东泽, 姚蓉, 等. 脓毒症相关凝血-炎症评分的构建及其对脓毒症预后评估效能分析[J]. 华西医学, 2018, 33(11): 1388-1394.
[25] Akca S, Haji-Michael P, de Mendonça A, et al. Time course of platelet counts in critically ill patients[J]. Crit Care Med, 2002, 30(4): 753-756. doi: 10.1097/00003246-200204000-00005
[26] Giustozzi M, Ehrlinder H, Bongiovanni D, et al. Coagulopathy and sepsis: Pathophysiology, clinical manifestations and treatment[J]. Blood Rev, 2021, 50: 100864. doi: 10.1016/j.blre.2021.100864
[27] 朱为民, 黄丹红, 王巧红, 等. 脓毒症诱导凝血功能障碍对脓毒症患者预后的评估价值[J]. 中华急诊医学杂志, 2023, 32(6): 781-786.
[28] 王子文, 赵文静, 晁亚丽. D-二聚体、乳酸联合可溶性血小板内皮黏附分子-1对脓毒症相关弥散性血管内凝血患者预后不良的预测研究[J]. 实用医学杂志, 2023, 39(18): 2379-2383.
[29] 印明珠, 孙明, 燕宪亮. 血栓弹力图、凝血功能与平均血小板体积/血小板计数比值的联合监测对脓毒症患者预后的评估[J]. 中华急诊医学杂志, 2022, 31(10): 1347-1352.
[30] 彭松, 贺莉, 武欣迎, 等. D-二聚体对新型冠状病毒肺炎患者病情严重程度及预后的评估价值[J]. 实用医学杂志, 2020, 36(17): 2321-2324.
[31] 张连钰, 张发斌, 白焕英, 等. 高原地区颅脑损伤患者血清降钙素原水平与病情严重程度及预后的关联研究[J]. 中华危重病急救医学, 2024, 36(1): 56-61.
[32] 刘慧琳, 傅义程, 郝靖欣, 等. 血清降钙素原水平和APACHEⅡ评分对老年脓毒症患者预后的预测价值分析[J]. 中华危重病急救医学, 2023, 35(1): 56-60.
[33] 张艳, 尚楠, 贺婷, 等. 脓毒症心肌损伤患者中降钙素原与短期预后的相关性分析[J]. 中华心力衰竭和心肌病杂志, 2023, 7(4): 334-338.
-
计量
- 文章访问数: 74
- 施引文献: 0