
Analysis of influencing factors of persistent inflammation and immunosuppression and catabolism syndrome after severe trauma
-
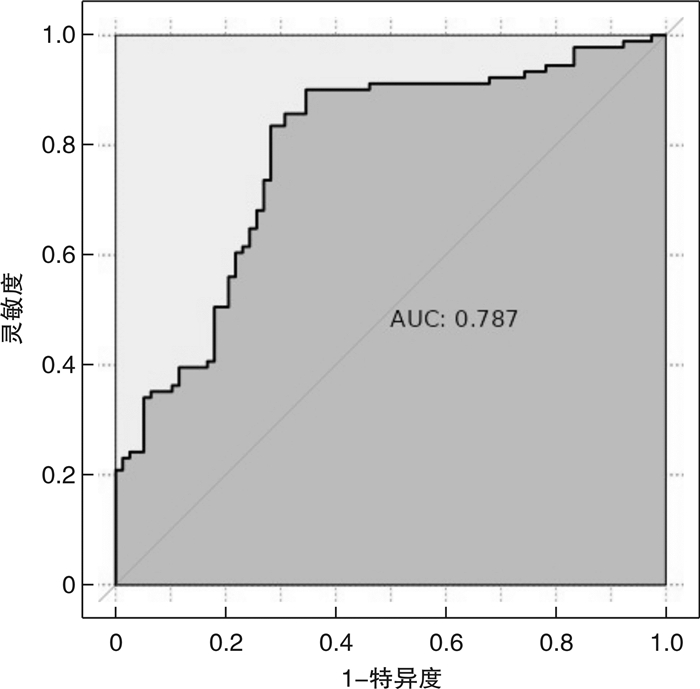
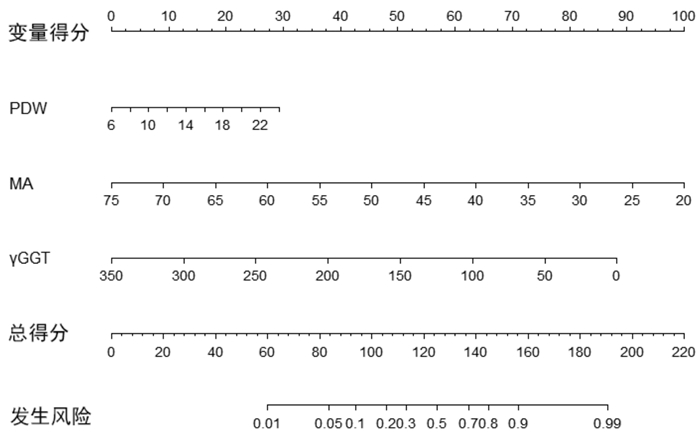
摘要: 目的 研究严重创伤进展为持续炎症-免疫抑制-分解代谢综合征(persistent inflammation,immunosuppression and catabolism syndrome,PICS)的影响因素,并构建PICS发生风险的列线图预测模型并评估其预测效果。方法 收集新疆医科大学第一附属医院TICU 2017年6月—2023年5月收治的169例严重创伤患者资料。根据ICU住院第14天的C反应蛋白、淋巴细胞计数和白蛋白水平将患者分为PICS组(78例)和非PICS组(91例)。收集了患者的入院初次诊断指标、血栓弹力图、血小板指标及生化指标,使用独立样本t检验、Mann-WhitneyU检验和χ2检验进行单因素分析,再进行多因素logistic分析确定严重创伤并发PICS的危险因素;使用R软件建立列线图预测模型,通过受试者工作特征曲线下面积(area under curve,AUC)和拟合度检验评估模型预测效果。结果 在169例严重创伤患者中,78例发展为PICS,91例未发展为PICS。两组在年龄、年龄评分、最大振幅(maximum amplitude,MA)、凝固角、血块30 min溶解百分比、血液凝固时间、血小板平均分布宽度、血小板计数、血小板压积、总蛋白、球蛋白、总胆固醇及γ谷氨酰胺基转肽酶(γ-glutamyl transferase,γ-GGT)方面差异有统计学意义(P<0.05)。多因素logistic回归分析显示,血小板平均分布宽度(platelet distribution width,PDW)、MA、γ-GGT是严重创伤并发PICS的独立影响因素(H-L检验0.847,正确百分比74%),使用这些独立危险因素建立的列线图模型具有较好区分度及校准度(AUC=0.787,MAE=0.053)。结论 PDW、MA、γ-GGT是严重创伤并发PICS的独立影响因素。基于这些指标构建的列线图模型能较好预测严重创伤患者发生PICS的可能性,有助于早期识别和阻止PICS的发生发展。
-
关键词:
- 严重创伤 /
- 持续炎症-免疫抑制-分解代谢综合征 /
- 血栓弹力图 /
- 列线图
Abstract: Objective To investigate the factors affecting the progression of severe trauma to persistent inflammation, immunosuppression and catabolism syndrome(PICS), and to construct a nomogram prediction model for the risk of PICS and evaluate its predictive effect.Methods The data of 169 patients with severe trauma treated in TICU of the first affiliated Hospital of Xinjiang Medical University from June 2017 to May 2023 were collected, including 136 males and 33 females. The patients were divided into PICS group(n=78) and non-PICS group(n=91) according to the C-reactive protein, lymphocyte and albumin levels on the 14th day of ICU stay in hospital. The initial diagnostic indexes, thrombelastography, platelet related indexes and biochemical indexes were collected, and the basic data and the above test results of the two groups were compared respectively. Independent samplettest, Mann-WhitneyUtest andχ2 test were used for univariate analysis, and multivariate logistic regression analysis was used to analyze the risk factors of severe trauma complicated with PICS. A nomogram prediction model was established by R software, and the effect of the model was tested according to the area under the curve(AUC) and the degree of fit of the receiver operating characteristic.Results The age, age score, estimate percent lysis, K, platelet distribution width(PDW), maximum amplitude(MA), Angle, platelet, plateletcrit, total protein, GLOB, TC and γ-GGT were significantly different between the two groups. Multivariate logistic regression analysis showed that PDW, MA and γ-GGT were independent risk factors of severe trauma complicated with PICS(H-L test=0.847, correct percentage=74%). The nomogram model established with these independent risk factors has a good degree of differentiation and calibration(AUC=0.787, MAE=0.053).Conclusion PDW, MA and γ-GGT are independent risk factors of severe trauma complicated with PICS. The nomogram model established based on these indexes can better predict the possibility of PICS in patients with severe trauma and help to identify and prevent the occurrence and development of PICS in the early stage. -

-
表 1 严重创伤并发PICS的患者基本特征资料
X±S,M(P25,P75) 指标 PICS组(78例) 非PICS组(91例) χ2/t/Z P 性别/例(%) 1.582 0.209 男 66(85) 70(77) 女 12(15) 21(23) 年龄/岁 54.23(40.75,67.00) 47.97(36.00,50.00) -2.254 0.024 ISS评分/分 39.47±10.41 37.80±11.45 0.994 0.332 GCS评分/分 9.68±4.22 9.60±4.46 0.112 0.911 APACHEⅡ评分/分 16.00(11.75,20.00) 14.00(10.00,20.00) -0.594 0.553 急性评分/分 10.00(5.00,13.00) 10.00(5.00,14.00) -0.196 0.845 慢性评分/分 3.10±2.43 3.34±1.95 -0.707 0.488 年龄评分/分 2.63±2.13 1.96±2.01 2.103 0.036 损伤部位/例(%) 0.323 0.851 头颈部 33(42) 36(40) 多发伤 37(47) 47(52) 其他部位a) 8(11) 8(8) 受伤机制/例(%) 5.158 0.161 车祸 46(59) 41(45) 摔伤 12(15) 21(23) 坠落 10(13) 20(22) 其他b) 10(13) 9(10) a)其他部位为胸部、腹部、四肢及骨盆,其中PICS组分别为2、2、2、2例,非PICS组分别为4、1、3、0例。b)其他为锐器伤、殴打伤、烧烫伤、电击伤及挤压伤,其中PICS组分别为2、2、1、0、5例,非PICS组分别为0、1、2、1、5例。  下载: 导出CSV
下载: 导出CSV
表 2 PICS组与非PICS组入院初次检验结果的单因素比较分析
X±S,M(P25,P75) 因素 PICS组(78例) 非PICS组(91例) t/Z P 初次诊断指标 CRP/(mg/L) 53.02±68.21 70.05±127.65 -1.102 0.272 LYM/(×109/L) 1.20±1.39 1.58±1.83 -1.53 0.128 ALB/(g/L) 33.33±7.67 35.20±7.54 -1.594 0.113 TEG指标 LY30/% 0.06±0.17 0.06±0.17 -0.044 0.965 EPL/% 0.13±0.31 0.06±0.10 2.155 0.046 MA/mm 53.58±6.13 58.77±6.62 -5.29 <0.001 Angle/deg 63.78±7.25 67.94±6.52 -3.89 <0.001 K/min 2.28±1.87 1.69±0.81 2.621 0.010 R/min 4.72±0.94 4.87±1.22 -0.915 0.362 血小板指标 PLT/(×109/L) 173(117,222) 197(149,255) -2.279 0.023 MPV/fL 10.00(9.20,10.73) 10.00(9.20,10.70) -0.259 0.796 PCT/% 0.17±0.06 0.21±0.10 -3.154 0.002 PDW/% 12.31±3.20 11.03±2.36 2.997 0.003 生化指标 TG/(mmol/L) 1.43±1.56 2.06±5.22 -1.094 0.276 HDL/(mmol/L) 0.88(0.70,1.08) 0.87(0.62,1.16) -0.145 0.885 LDL/(mmol/L) 1.86±0.84 2.23±1.56 -1.946 0.054 TP/(g/L) 58.86(49.28,67.52) 63.94(30.69,41.6) 2.250 0.020 GLOB/(g/L) 24.72(21.25,29.56) 27.78(22.71,31.82) 2.600 0.010 A/G 2.97±14.00 1.27±0.30 1.160 0.248 TC/(mmol/L) 3.15±1.08 3.56±1.34 -2.187 0.030 γ-GGT/(U/L) 44.24±50.90 25.54±17.09 3.295 <0.001
下载: 导出CSV
表 3 严重创伤并发PICS的多因素logistic回归分析
因素 B SE OR 95%CI P 年龄 -0.038 0.028 0.962 0.911~1.017 0.171 年龄评分 0.108 0.231 1.114 0.708~1.751 0.641 EPL -1.396 1.027 0.247 0.033~1.853 0.174 MA 0.117 0.055 1.125 1.009~1.253 <0.05 Angle 0.059 0.055 1.060 0.952~1.181 0.285 K 0.363 0.245 1.438 0.89~2.322 0.138 PLT -0.013 0.009 0.987 0.971~1.004 0.135 PCT 11.494 9.340 98 124.645 0.001~8.743 0.218 PDW -0.176 0.089 0.838 0.704~0.999 <0.05 TP -0.029 0.030 0.972 0.916~1.031 0.339 GLOB 0.079 0.056 1.082 0.969~1.208 0.159 TC 0.043 0.205 1.044 0.698~1.561 0.833 γ-GGT 0.016 0.008 1.017 1.000~1.033 <0.05 常量 -7.860 4.052 0 0.052
下载: 导出CSV
-
[1] Wendlandt B, Ceppe A, Cox CE, et al. The Association between Patient Health Status and Surrogate Decision Maker Post-Traumatic Stress Disorder Symptoms in Chronic Critical Illness[J]. Ann Am Thorac Soc, 2021, 18(11): 1868-1875. doi: 10.1513/AnnalsATS.202010-1300OC
[2] Efron PA, Brakenridge SC, Mohr AM, et al. The Persistent Inflammation, Immunosuppression, and Catabolism Syndrome(PICS)Ten Years Later[J]. J Trauma Acute Care Surg, 2023.
[3] Gentile LF, Cuenca AG, Efron PA, et al. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care[J]. J Trauma Acute Care Surg, 2012, 72(6): 1491-501. doi: 10.1097/TA.0b013e318256e000
[4] 姜海, 陈练, 赵扬玉. 凝血-免疫-炎症交互作用与产后出血关系的研究进展[J]. 中华妇产科杂志, 2021, 56(2): 149-152.
[5] 蒋炫东, 张为民, 方强. 两种评分预测持续炎症-免疫抑制-分解代谢综合征患者死亡的效能比较[J]. 浙江医学, 2022, 44(1): 33-37. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJYE202201008.htm
[6] 唐庭轩, 唐良晟, 陈登, 等. 严重多发伤患者并发持续炎症-免疫抑制-分解代谢综合征的早期警示因子[J]. 中华急诊医学杂志, 2022, 31(5): 598-602. doi: 10.3760/cma.j.issn.1671-0282.2022.05.005
[7] 李娅, 王铭, 李辉凤, 等. 年龄联合CD4+与CD8+比值对多发伤并发持续炎症-免疫抑制-分解代谢综合征的预测价值[J]. 中国急救医学, 2021, 41(11): 932-937. doi: 10.3969/j.issn.1002-1949.2021.11.003
[8] 国家创伤医学中心, 中国创伤救治联盟. 严重创伤患者院前急救规范T/CADERM 3040-2020[S]. 北京: 中国医学救援协会, 2020: 6.
[9] Kanda N, Ohbe H, Nakamura K. Effects of Antithrombin on Persistent Inflammation, Immunosuppression, and Catabolism Syndrome among Patients with Sepsis-Induced Disseminated Intravascular Coagulation[J]. J Clin Med, 2023, 12(11): 3822. doi: 10.3390/jcm12113822
[10] 刘云涛, 李俊, 王大伟, 等. 脓毒症并发PICS的早期临床特征及相关影响因素分析[J]. 广州中医药大学学报, 2021, 38(3): 441-448. https://www.cnki.com.cn/Article/CJFDTOTAL-REST202103002.htm
[11] 李辉凤, 王铭, 潘险峰. 持续炎症-免疫抑制-分解代谢综合征研究新进展[J]. 临床急诊杂志, 2022, 23(3): 219-224. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.03.012
[12] Celegen M, Kesici S, Yavuz S, et al. Are platelet indices promising ratios for predicting pediatric septic shock prognosis?[J]. Bratisl Lek Listy, 2022, 123(6): 444-448.
[13] 李俊玉, 王雅慧, 刘慧珍, 等. 红细胞分布宽度与血小板计数比值对急诊脓毒症患者预后的预测价值[J]. 临床急诊杂志, 2022, 23(2): 132-137. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.02.011
[14] 张涛, 万亚楠, 卢昕媛, 等. 血栓弹力图对脓毒症患者弥散性血管内凝血的诊断价值及预后的影响[J]. 临床急诊杂志, 2022, 23(7): 476-481. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.07.004
[15] Matthay Z A, Kornblith LZ. Platelet Contributions to Trauma-Induced Coagulopathy: Updates in Post-injury Platelet Biology, Platelet Transfusions, and Emerging Platelet-Based Hemostatic Agents[J]. Current Trauma Reports, 2019, 62(5): 202-209.
[16] 苏和毅, 莫泽珣, 刘星, 等. 内科重症监护病房中继发持续性炎症-免疫抑制-分解代谢综合征的老年脓毒症患者回顾性分析[J]. 中华老年医学杂志, 2019, 38(8): 869-874.
[17] Mandel J, Casari M, Stepanyan M, et al. Beyond Hemostasis: Platelet Innate Immune Interactions and Thromboinflammation[J]. Int J Mol Sci, 2022, 23(7): 3868.
[18] Wong CH, Jenne CN, Petri B, et al. Nucleation of platelets with blood-borne pathogens on Kupffer cells precedes other innate immunity and contributes to bacterial clearance[J]. Nat Immunol, 2013, 14(8): 785-792.
[19] Severin S, Gratacap MP, Bouvet L, et al. Phosphoinositides take a central stage in regulating blood platelet production and function[J]. Adv Biol Regul, 2023, 2023: 100992.
[20] Ping L, Gao Y, He Y, et al. Systematic Oxidative Stress Indexes Associated with the Prognosis in Patients with T Lymphoblastic Lymphoma/Leukemia[J]. Oxid Med Cell Longev, 2022, 2022: 2679154.
[21] 代冬梅, 唐仕宇, 许汪斌, 等. 妊娠期急性脂肪肝与HELLP综合征患者临床特征比较[J]. 中华危重病急救医学, 2022, 34(6): 624-629. https://cdmd.cnki.com.cn/Article/CDMD-10678-1022096366.htm
[22] Sawada K, Shimomura Y, Hasegawa D, et al. Association of circulating histone H3 and high mobility group box 1 levels with postoperative prognostic indicators in intensive care unit patients: a single-center observational study[J]. Fujita Med J, 2023, 9(2): 95-100.
[23] Deng S, Zheng Y, Mo Y, et al. Ferroptosis Suppressive Genes Correlate with Immunosuppression in Glioblastoma[J]. World Neurosurg, 2021, 152: e436-e448.
[24] Kim R, Hashimoto A, Markosyan N, et al. Ferroptosis of tumour neutrophils causes immune suppression in cancer[J]. Nature, 2022, 612(7939): 338-346.
[25] Liu Y, Zhang Y, Wang C, et al. Inhibition of DDX3X alleviates persistent inflammation, immune suppression and catabolism syndrome in a septic mice model[J]. Int Immunopharmacol, 2023, 117: 109779.
[26] 李医华, 文韬, 千永日, 等. 健康体检者血尿酸和γ-谷氨酰转肽酶水平与代谢综合征的关联性分析[J]. 吉林大学学报(医学版), 2022, 48(6): 1605-1613. https://www.cnki.com.cn/Article/CJFDTOTAL-BQEB202206029.htm
[27] 白丽爽, 王兴义, 杨立山. 多发伤患者预后列线图模型的构建和研究[J]. 中华急诊医学杂志, 2023, 32(4): 540-545. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGYG202211012.htm
-

图(3)
表(3)
计量
- 文章访问数: 999
- PDF下载数: 196
- 施引文献: 0