
Comparison of long-term survival in patients with risky EGVB treated by different surgical methods and its influencing factors
-
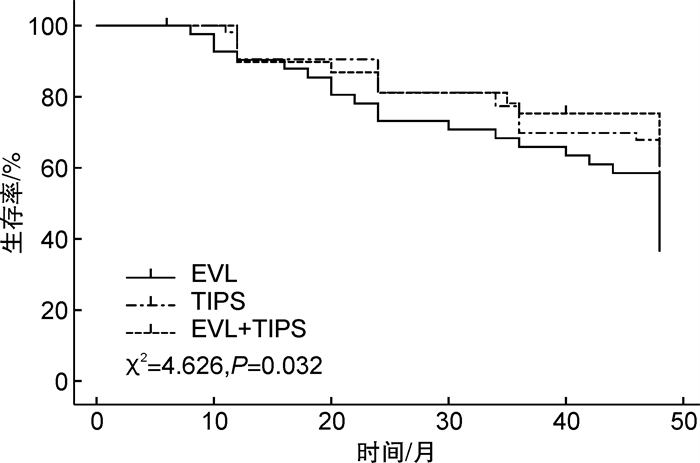
摘要: 目的 研究不同术式治疗危险性食管胃底静脉曲张破裂出血(esophageal-gastric varices bleeding, EGVB)患者远期生存状况比较及其影响因素分析。方法 回顾性研究选取2019年3月-2022年9月期间邢台医学高等专科学校第二附属医院收治的135例肝硬化合并EGVB患者, 均行手术治疗, 其中42例套扎术(套扎术组)、54例分流术(Tips组)和39例套扎术及分流术(联合组), 随访至2023年3月, 比较3种手术方式患者的临床疗效、肝功能指标、再出血率和远期生存率期。采集肝硬化并发EGVB患者基线资料, 根据患者随访结果, 将患者分成死亡组(62例)和存活组(73例), 单因素分析和Cox回归分析确定EGVB患者远期死亡的影响因素。结果 联合组患者临床总效率为92.31%, 明显高于套扎术组的78.57%和Tips组的70.37%, 但套扎术组和Tips组患者临床总有效率差异无统计学意义。Tips组和联合组患者术后1个月TBiL和ALT数值明显高于套扎术组, Tips组和联合组患者术后6个月ALT明显高于套扎术组。3组患者均发生切口感染、肺部感染、吞咽困难、腹腔积液等并发症, 差异无统计学意义。套扎术组患者术后1个月再出血发生率为14.29%, 高于Tips组的7.41%和联合组的5.13%;套扎术组患者术后6个月再出血发生率为19.05%, 高于Tips组的12.96%和联合组的7.69%, 差异无统计学意义(P>0.05)。联合组患者远期生存率为66.67%, 明显高于Tips组的57.41%和套扎术组的38.10%, 差异有统计学意义(χ2=4.626, P=0.032)。死亡组和存活组患者在年龄、6个月内再出血、消化道出血史、Child-pugh分级、中性粒细胞、白细胞计数、终末期肝病模型(Model for end-stage liver disease, MELD)评分总分及治疗方式等指标差异有统计学意义(P < 0.05)。Cox回归分析结果显示, 6个月内再出血(OR=2.028, 95%CI: 1.289~3.189)、Child-Pugh分级(OR=1.505, 95%CI: 1.041~2.176)、白细胞计数(OR=1.721, 95%CI: 1.379~2.148)、MELD总分(OR=6.135, 95%CI: 3.296~11.419)和治疗方式(OR=5.058, 95%CI: 1.779~14.378)是影响EGVB患者死亡的影响因素。结论 分流术应用于肝硬化合并危险性EGVB疾病可有效提高临床疗效, 且联合套扎术可延长远期生存, 且6个月内再出血、Child-Pugh分级、白细胞计数、MELD总分及治疗方式可应用于预测EGVB患者死亡, 临床应根据其指标水平积极制定干预措施, 以降低患者死亡率。
-
关键词:
- 食管胃底静脉曲张破裂出血 /
- 肝硬化 /
- 治疗方式 /
- 远期生存 /
- 影响因素
Abstract: Objective To explore the comparison of long-term survival in patients with risky esophageal-gastric varices bleeding treated by different surgical methods and the influencing factors.Methods In a retrospective study, 135 patients with liver cirrhosis and esophageal-gastric varices bleeding admitted to a hospital between March 2019 and September 2022 were included, all of whom underwent surgical treatment. Among them, 42 patients underwent ligation, 54 underwent shunt surgery, and 39 underwent both ligation and shunt surgery. Follow-up was conducted until March 2023, comparing the clinical efficacy, liver function indicators, rebleeding rate, and long-term survival of patients undergoing the three surgical methods. Baseline data of patients with liver cirrhosis complicated by esophageal-gastric varices bleeding were collected, and patients were divided into a deceased group(n=62) and a survival group(n=73) based on follow-up results. Univariate analysis and Cox regression analysis were employed to determine the influencing factors of long-term mortality in esophageal-gastric varices bleeding patients.Results In this study, the combined treatment group(ligation and shunt) demonstrated a notably higher overall clinical efficacy rate of 92.31% compared to the ligation group(78.57%) and the shunt group(70.37%). However, no statistically significant difference was observed between the clinical efficacy rates of the ligation and shunt groups(P>0.05). The total bilirubin (TBiL) and alanine aminotransferase (ALT) levels in both the shunt and combined groups were significantly elevated compared to the ligation group one month after surgery. Additionally, the ALT levels in the shunt and combined groups remained significantly higher than the ligation group six months after surgery. Incision infection, lung infection, dysphagia, peritoneal effusion and other complications occurred in all three groups, and the differences were not statistically significant. The one-month postoperative rebleeding rate was higher in the ligation group(14.29%) compared to the shunt group(7.41%) and the combined group(5.13%). Similarly, the six-month postoperative rebleeding rate was higher in the ligation group(19.05%) compared to the shunt group(12.96%) and the combined group(7.69%), although these differences were not statistically significant(P>0.05). The long-term survival rate for the combined treatment group was 66.67%, which was significantly higher than the shunt group(57.41%) and the ligation group(38.10%), with a statistically significant difference(χ2=4.626, P=0.032). Significant statistical differences were found between the deceased group and the survival group in terms of age, rebleeding within 6 months, history of gastrointestinal bleeding, Child-Pugh classification, neutrophils, white blood cell count, Model for end-stage liver disease(MELD) total score, and treatment methods(P < 0.05). Cox regression analysis results showed that rebleeding within 6 months(OR=2.028, 95%CI: 1.289-3.189), Child-Pugh classification(OR=1.505, 95%CI: 1.041-2.176), white blood cell count(OR=1.721, 95%CI: 1.379-2.148), MELD total score(OR=6.135, 95%CI: 3.296-11.419), and treatment methods(OR=5.058, 95%CI: 1.779-14.378) were influencing factors for the mortality of esophageal-gastric varices bleeding patients.Conclusion In patients with cirrhosis and high-risk esophageal and gastric variceal bleeding, shunt surgery significantly improves clinical outcomes and, when combined with banding ligation, prolongs long-term survival. Additionally, factors such as rebleeding within six months, Child-Pugh classification, leukocyte count, MELD total score, and treatment approaches can be utilized to predict mortality in esophageal-gastric varices bleeding patients. Consequently, it is crucial for clinicians to develop personalized intervention strategies based on these prognostic indicators to reduce patient mortality. -

-
表 1 3组患者临床疗效比较
组别 显效/例 有效/例 无效/例 临床总有效率/例(%) 套扎术组(42例) 21 12 9 33(78.57)1) Tips组(54例) 17 21 16 38(70.37)1) 联合组(39例) 25 11 3 36(92.31) χ2 6.647 P 0.036 与联合组比较,1)P < 0.05。  下载: 导出CSV
下载: 导出CSV
表 2 3组患者肝功能TBiL比较
μmol/L,X±S 组别 治疗前 术后1个月 术后6个月 套扎术组(42例) 28.87±4.23 27.81±3.91 28.01±4.52 Tips组(54例) 28.50±5.15 34.12±4.871) 30.21±4.33 联合组(39例) 28.41±4.88 34.58±5.031) 29.03±5.09 F 0.108 28.493 2.710 P 0.897 < 0.001 0.070 与套扎术组比较,1)P < 0.01。
下载: 导出CSV
表 3 3组患者肝功能ALT比较
U/L,X±S 组别 治疗前 术后1个月 术后6个月 套扎术组(42例) 37.88±5.35 45.02±6.17 40.02±4.22 Tips组(54例) 37.56±4.77 62.87±8.011) 45.42±3.431) 联合组(39例) 38.10±5.02 63.00±7.851) 46.87±4.081) F 0.136 83.827 36.286 P 0.873 < 0.001 < 0.001 与套扎术组比较,1)P < 0.01。
下载: 导出CSV
表 4 3组患者肝功能ALB比较
g/L,X±S 组别 治疗前 术后1个月 术后6个月 套扎术组(42例) 32.81±4.34 31.86±4.18 31.23±5.01 Tips组(54例) 31.76±5.00 32.09±5.02 31.89±6.17 联合组(39例) 32.59±4.87 30.87±4.76 31.54±5.24 F 0.657 0.816 0.167 P 0.520 0.445 0.846
下载: 导出CSV
表 5 3组患者术后并发症比较
例 组别 切口
感染肺部
感染吞咽
困难腹腔
积液套扎术组(42例) 2 3 5 9 Tips组(54例) 3 2 3 8 联合组(39例) 3 4 2 8 χ2 0.334 1.585 1.804 0.829 P 0.846 0.453 0.406 0.661
下载: 导出CSV
表 6 3组患者再出血发生率比较
例(%) 组别 术后1个月 术后6个月 套扎术组(42例) 6(14.29) 8(19.05) Tips组(54例) 4(7.41) 7(12.96) 联合组(39例) 2(5.13) 3(7.69) χ2 2.338 2.267 P 0.311 0.322
下载: 导出CSV
表 7 肝硬化合并EGVB患者死亡的单因素分析
例 基线资料 例数 死亡组
(62例)存活组
(73例)χ2/t P 基线资料 例数 死亡组
(62例)存活组
(73例)χ2/t P 性别 3.682 0.055 肝性脑病 1.814 0.178 男 91 47 44 有 34 19 15 女 44 15 29 无 101 43 58 年龄/岁 8.855 0.012 消化道出血史 4.910 0.027 < 35 37 12 25 有 109 45 64 35~65 54 22 32 无 26 17 9 >65 44 28 16 Child-pugh分级 10.309 0.006 6个月内再出血 11.703 0.001 A 8 1 7 有 18 15 3 B 34 10 24 无 117 47 70 C 93 51 42 肝硬化病因 5.679 0.059 中性粒细胞/% 135 78.35± 76.23± 2.060 0.041 酒精性 51 17 34 6.41 5.55 病毒性 59 33 26 白细胞计数/(×109/L) 135 8.67± 5.79± 22.162 < 0.001 酒精性和病毒性 25 12 13 0.81 0.70 糖尿病 0.121 0.728 MELD总分/分 135 65.79± 61.17± 4.200 < 0.001 有 16 8 8 7.22 5.19 无 119 54 65 治疗方式 7.050 0.030 高血压 0.139 0.710 套扎术 42 26 16 有 18 9 9 分流术 54 23 31 无 117 53 64 套扎术+分流术 39 13 26
下载: 导出CSV
表 8 变量赋值
因素 变量 赋值 随访结束是否死亡 Y “存活”=0,“死亡”=1 年龄 X1 “ < 35岁”=1;“35~65岁”=2;“>65岁”=3 6个月内再出血 X2 “否”=1,“是”=2 消化道出血史 X3 “否”=1,“是”=2 Child-Pugh分级 X4 “A”=1;“B”=2;“C”=3 中性粒细胞 X5 连续变量 白细胞计数 X6 连续变量 MELD总分 X7 连续变量 治疗方式 X8 “联合治疗”=1;“分流术”=2;“套扎术”=3
下载: 导出CSV
表 9 肝硬化合并EGVB死亡患者Cox分析结果
因素 β SE Wald P OR 95%CI 6个月内再出血 0.707 0.231 9.367 0.002 2.028 1.289~3.189 Child-Pugh分级 0.409 0.188 4.733 0.030 1.505 1.041~2.176 白细胞计数 0.543 0.113 23.091 < 0.001 1.721 1.379~2.148 MELD总分 1.814 0.317 32.746 < 0.001 6.135 3.296~11.419 治疗方式 1.621 0.533 9.249 < 0.001 5.058 1.779~14.378 常数项 -0.762 0.102 55.810 < 0.001
下载: 导出CSV
-
[1] Gralnek IM, Camus Duboc M, Garcia-Pagan JC, et al. Endoscopic diagnosis and management of esophagogastric variceal hemorrhage: European Society of Gastrointestinal Endoscopy(ESGE)Guideline[J]. Endoscopy, 2022, 54(11): 1094-1120. doi: 10.1055/a-1939-4887
[2] 屠军, 李慧瑛, 李峰, 等. 肝硬化食管胃静脉曲张出血患者并发肝性脑病危险因素的临床分析[J]. 中国中西医结合消化杂志, 2020, 28(7): 552-555. doi: 10.3969/j.issn.1671-038X.2020.07.16
[3] Osman KT, Nayfeh T, Abdelfattah AM, et al. Secondary prophylaxis of gastric variceal bleeding: a systematic review and network meta-analysis[J]. Liver Transpl, 2022, 28(6): 945-958. doi: 10.1002/lt.26383
[4] Lee HA, Kwak J, Cho SB, et al. Endoscopic variceal obturation and retrograde transvenous obliteration for acute gastric cardiofundal variceal bleeding in liver cirrhosis[J]. BMC Gastroenterol, 2022, 22(1): 355. doi: 10.1186/s12876-022-02428-1
[5] Luo X, Hernández-Gea V. Update on the management of gastric varices[J]. Liver Int, 2022, 42(6): 1250-1258. doi: 10.1111/liv.15181
[6] Villanueva C, Torres F, Sarin SK, et al. Carvedilol reduces the risk of decompensation and mortality in patients with compensated cirrhosis in a competing-risk meta-analysis[J]. J Hepatol, 2022, 77(4): 1014-1025. doi: 10.1016/j.jhep.2022.05.021
[7] Liu CH, Liu S, Zhao YB, et al. Development and validation of a nomogram for esophagogastric variceal bleeding in liver cirrhosis: A cohort study in 1099 cases[J]. J Dig Dis, 2022, 23(10): 597-609. doi: 10.1111/1751-2980.13145
[8] Lai M, Afdhal NH. Liver Fibrosis Determination[J]. Gastroenterol Clin North Am, 2019, 48(2): 281-289. doi: 10.1016/j.gtc.2019.02.002
[9] 中华医学会肝病学分会, 中华医学会消化病学分会, 中华医学会内镜学分会. 肝硬化门静脉高压食管胃静脉曲张出血的防治指南[J]. 临床肝胆病杂志, 2016, 32(2): 203-219. doi: 10.3969/j.issn.1001-5256.2016.02.002
[10] DuBrock HM, Del Valle KT, Krowka MJ. Mending the Model for End-Stage Liver Disease: An in-depth review of the past, present, and future portopulmonary hypertension Model for End-Stage Liver Disease exception[J]. Liver Transpl, 2022, 28(7): 1224-1230. doi: 10.1002/lt.26422
[11] Dias E, Marques M, Macedo G. Endoscopic management of esophageal and gastric lesions with underlying varices[J]. Ann Gastroenterol, 2022, 35(5): 452-461.
[12] 史东阳, 肖玲燕, 杨凯, 等. 液体平衡对肝硬化合并肝性脑病患者短期预后的影响[J]. 临床急诊杂志, 2022, 23(10): 733-737. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.10.009
[13] Jakab SS, Garcia-Tsao G. Evaluation and management of esophageal and gastric varices in patients with cirrhosis[J]. Clin Liver Dis, 2020, 24(3): 335-350. doi: 10.1016/j.cld.2020.04.011
[14] Villanueva C, Torres F, Sarin SK, et al. Carvedilol reduces the risk of decompensation and mortality in patients with compensated cirrhosis in a competing-risk meta-analysis[J]. J Hepatol, 2022, 77(4): 1014-1025. doi: 10.1016/j.jhep.2022.05.021
[15] Boike JR, Thornburg BG, Asrani SK, et al. North American Practice-Based Recommendations for Transjugular Intrahepatic Portosystemic Shunts in Portal Hypertension[J]. Clin Gastroenterol Hepatol, 2022, 20(8): 1636-1662.
[16] Lv Y, Chen H, Luo B, et al. Concurrent large spontaneous portosystemic shunt embolization for the prevention of overt hepatic encephalopathy after TIPS: A randomized controlled trial[J]. Hepatology, 2022, 76(3): 676-688. doi: 10.1002/hep.32453
[17] Giri S, Sundaram S, Jearth V, et al. Predictors of early bleeding after endoscopic variceal ligation for esophageal varices: a systematic review and meta-analysis[J]. Clin Exp Hepatol, 2022, 8(4): 267-277.
[18] Singh V, Kumar P, Verma N, et al. Propranolol vs. band ligation for primary prophylaxis of variceal hemorrhage in cirrhotic patients with ascites: a randomized controlled trial[J]. Hepatol Int, 2022, 16(4): 944-953. doi: 10.1007/s12072-022-10361-4
[19] Broussard KA, Rockey DC. Bleeding ectopic varices: clinical presentation, natural history, and outcomes[J]. J Investig Med, 2022, 70(5): 1280-1284.
[20] Seven G, Musayeva G, Seven OO, et al. Comparison of endoscopic ultrasound-guided coil deployment with and without cyanoacrylate injection for gastric varices[J]. Arab J Gastroenterol, 2022, 23(2): 115-119.
[21] Gao Z, Li S, Zhao J, et al. Anticoagulation therapy early is safe in portal vein thrombosis patients with acute variceal bleeding: a multi-centric randomized controlled trial[J]. Intern Emerg Med, 2023, 18(2): 513-521.
[22] Tranah TH, Ballester MP, Carbonell-Asins JA, et al. Plasma ammonia levels predict hospitalisation with liver-related complications and mortality in clinically stable outpatients with cirrhosis[J]. J Hepatol, 2022, 77(6): 1554-1563.
[23] 黄飞, 祁玮, 何健, 等. 感染部位与发生脓毒症肝损伤的相关性研究[J]. 临床急诊杂志, 2021, 22(10): 653-656. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2021.10.003
-
图(1)
表(9)
计量
- 文章访问数: 334
- PDF下载数: 130
- 施引文献: 0