
Correlation analysis of sST2 and poor prognosis in patients with intravenous thrombolysis in acute ischemic stroke
-
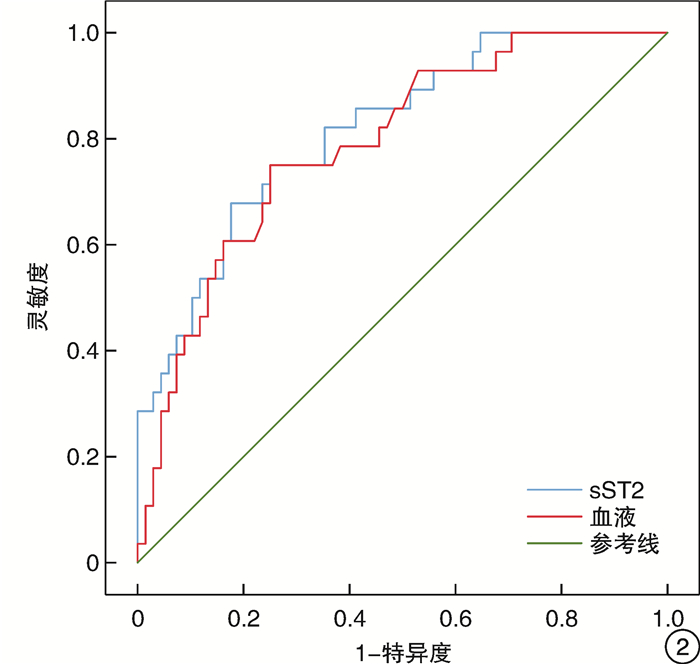
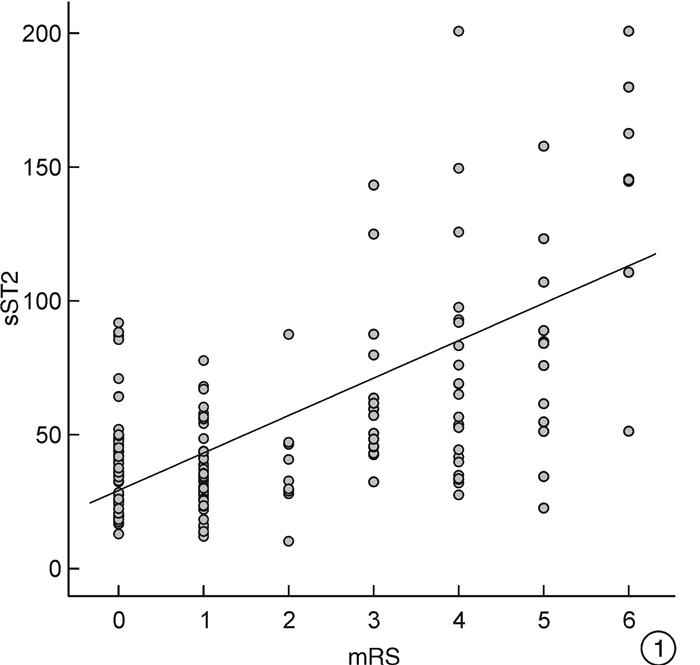
摘要: 目的 分析接受重组组织型纤溶酶原激活剂(recombinant tissue plasminogen activator,rt-PA)静脉溶栓治疗的急性缺血性卒中(acute ischemic stroke,AIS)患者预后不良与可溶性生长刺激表达基因2蛋白(soluble growth stimulating expression gene 2,sST2)的相关性。方法 纳入接受rt-PA静脉溶栓治疗的AIS患者96例,入院后记录所有患者的一般资料,美国国立卫生研究院卒中量表(National Institutes of Health Stroke scale,NIHSS)评分,发病至用药时间(onset-to-treatment time,OTT)以及是否发生溶栓后出血,检测sST2水平及其他实验室检查结果。溶栓后90 d采用改良Rankin量表(Modified Rankin scale,mRS)评估患者功能预后。分析影响AIS患者rt-PA静脉溶栓治疗预后不良的危险因素,并采用受试者工作特征(ROC)曲线评估sST2水平对其功能预后不良的预测价值。结果 单因素分析结果示:90 d预后不良组患者sST2水平高于预后良好组患者(P < 0.01)。多因素回归分析纳入相关混杂因素后结果表明,sST2为AIS患者rt-PA静脉溶栓治疗预后的独立危险因素(P < 0.05)。Spearman等级相关分析结果显示sST2水平与90 d mRS评分呈正相关。ROC曲线分析显示,sST2水平预测AIS患者rt-PA静脉溶栓治疗预后不良的灵敏度为67.9%,特异度为82.4%,曲线下面积(AUC)为0.816(95%CI:0.725~0.906,P < 0.01)。结论 sST2为接受rt-PA静脉溶栓治疗的AIS患者90 d预后不良的独立危险因素,对90 d预后不良具有较好的预测价值,可能是预测AIS患者rt-PA静脉溶栓治疗功能结局的潜在生物标志物。
-
关键词:
- 急性缺血性脑卒中 /
- 静脉溶栓 /
- 可溶性生长刺激表达基因2蛋白 /
- 重组组织型纤溶酶原激活剂 /
- 预后
Abstract: Objective To analyze the correlation between poor prognosis and soluble growth stimulating gene 2 protein(sST2) in patients with acute ischemic stroke(AIS) treated with recombinant tissue plasminogen activator(rt-PA) intravenous thrombolysis.Methods Ninety-six patients with AIS who received intravenous thrombolytic therapy with rt-PA were included. General information, National Institutes of Health Stroke scale (NIHSS) score, onset-to-medication time (OTT), and the occurrence of post-thrombolytic hemorrhage were recorded for all the patients after admission. The level of sST2 and other laboratory tests were measured. 90 days after thrombolysis, the functional prognosis of patients was evaluated using the Modified Rankin scale(mRS). To analyze the risk factors that affect the poor prognosis of patients with AIS after intravenous thrombolytic therapy with rt-PA, and to evaluate the predictive value of sST2 level on their poor functional prognosis using the subject performance characteristic(ROC) curve.Results The results of univariate analysis showed that the sST2 levels in patients with poor prognosis after 90 days were higher than those with good prognosis(P < 0.01). Multivariate regression analysis incorporating related confounding factors showed that sST2 was an independent risk factor for the prognosis of patients with AIS undergoing rt-PA intravenous thrombolysis therapy(P < 0.05). Spearman rank correlation analysis showed a positive correlation between the level of sST2 and the 90 day mRS score. ROC curve analysis showed that the sensitivity and specificity of sST2 level in predicting poor prognosis of patients with AIS after intravenous thrombolysis with rt-PA were 67.9%, 82.4%, and the area under curve(AUC) was 0.816(95%CI: 0.725-0.906, P < 0.01).Conclusion sST2 is an independent risk factor for poor prognosis in AIS patients receiving rt-PA intravenous thrombolytic therapy at 90 days, and has a good predictive value for poor prognosis at 90 days. It may be a potential biomarker for predicting the functional outcome of rt-PA intravenous thrombolytic therapy in AIS patients. -

-
表 1 90 d神经功能预后不良(mRS>2)的临床基线资料比较
变量 预后良好(68例) 预后不良(28例) χ2/Z/t P 年龄/岁 63.6±1.6 65.0±1.8 0.580 0.564 男性/例(%) 46(67.6) 23(82.1) 2.062 0.213 吸烟/例(%) 37(54.4) 16(57.1) 0.060 0.826 既往史/例(%) 高血压病 36(52.9) 18(64.3) 1.037 0.369 糖尿病 18(26.5) 9(32.1) 0.316 0.622 冠心病 11(16.2) 3(10.7) 0.475 0.751 心房颤动 10(14.7) 4(14.3) 0.003 0.958 高脂血症 18(26.5) 11(39.3) 1.545 0.230 高HCY血症 25(36.8) 16(57.1) 3.366 0.074 NIHSS评分 4(2~6) 11(5~15) 4.722 < 0.01 OTT/min 163±45 186±37 0.892 0.135 溶栓后出血/例(%) 4(5.9) 5(17.8) 0.739 < 0.01 实验室检测指标 sST2/(ng/mL) 34.5(26.8~44.1) 60.0(42.6~102.5) 4.844 < 0.01 血糖/(mmol/L) 5.2(4.6~6.3) 7.3(5.7~11.0) 4.446 < 0.01 糖化血红蛋白/% 5.9(5.4~6.6) 6.0(5.7~7.2) 1.115 0.265 白细胞计数/(109/L) 7.5±0.2 7.5±0.7 0.011 0.992 中性粒细胞计数/(109/L) 4.5(3.3~6.1) 4.1(5.1~8.7) 1.600 0.110 淋巴细胞计数/L 1.7±0.1 1.2±0.1 3.243 0.002 NLR 2.6(2.0~4.4) 5.2(3.2~9.9) 3.337 0.001 尿酸/(μmol/L) 287.0(240.1~362.8) 286.5(227.5~385.3) 0.282 0.778 D-二聚体 0.5(0.2~1.0) 0.6(0.2~1.6) 0.355 0.723 纤维蛋白原降解产物/(mg/L) 2.5(1.8~4.0) 2.5(1.8~5.5) 0.173 0.862  下载: 导出CSV
下载: 导出CSV
表 2 90 d神经功能预后不良(mRS>2)的多因素logistic回归分析
因素 β SE Wald χ2 OR(95%CI) P 高HCY血症 0.888 0.637 1.941 2.430(0.697~8.477) 0.164 NIHSS评分 0.110 0.057 3.672 1.116(0.998~1.248) 0.055 溶栓后出血 0.135 0.028 5.716 1.107(0.852~1.224) 0.084 sST2 0.042 0.016 6.828 1.362(1.093~1.697) 0.009 血糖 0.309 0.112 7.579 1.043(1.023~1.072) 0.006 淋巴细胞计数 -0.899 0.684 1.728 0.407(0.106~1.555) 0.189 NLR -0.036 0.138 0.069 0.964(0.736~1.264) 0.793 常量 -4.831 1.814 7.092 0.008 0.008 注:将单因素分析中P < 0.05的相关变量纳入多因素分析,即调整高HCY血症、NIHSS评分、溶栓后出血、血糖、淋巴细胞计数、NLR,所有自变量进入模型的方式为Enter。
下载: 导出CSV
-
[1] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-681. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004
[2] Wu H, Wu X, Chen S. Two mechanical thrombectomies in acute ischemic stroke within 48 hours: A case report on a patient with atrial fibrillation[J]. Radiol Case Rep, 2023, 18(9): 2995-2999. doi: 10.1016/j.radcr.2023.06.026
[3] 李丽灵, 马青峰. 急性脑梗死患者静脉溶栓后早期神经功能恶化的影响因素分析[J]. 中国脑血管病杂志, 2019, 16(12): 628-632. https://www.cnki.com.cn/Article/CJFDTOTAL-NXGB201912003.htm
[4] 石悦桐, 冯贵龙. 血清sST2与脑损伤的相关性研究进展[J]. 中国实用神经疾病杂志, 2021, 24(23): 2091-2098. https://www.cnki.com.cn/Article/CJFDTOTAL-HNSJ202123008.htm
[5] Lotierzo M, Dupuy AM, Kalmanovich E, et al. sST2 as avalue-added biomarker in heart failure[J]. Clin Chim Acta, 2020, 501(10): 120-130.
[6] Hansen C, Sastre C, Wolcott Z, et al. Time-dependent, dynamic prediction of fatty acid-binding protein 4, Galectin-3, and soluble ST2 measurement with poor outcome after acute stroke[J]. Int J Stroke, 2021, 16(6): 660-668. doi: 10.1177/1747493020971166
[7] 周婷, 花嵘, 陈令东, 等. Hcy、CysC、hs-CRP浓度在评估缺血性脑卒中患者功能预后中的价值[J]. 临床急诊杂志, 2021, 22(5): 347-351. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202105012.htm
[8] 王刚, 仲婷婷, 孙炎, 等. 免疫及炎性因子与急性缺血性卒中后神经损伤的相关性分析[J]. 临床急诊杂志, 2022, 23(2): 91-94. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.02.003
[9] Desai SM, Rocha M, Jovin TG, et al. High Variability in Neuronal Loss[J]. Stroke, 2019, 50(1): 34-37. doi: 10.1161/STROKEAHA.118.023499
[10] Mildner M, Storka A, Lichtenauer M, et al. Primary sources and immunological prerequisites for sST2 secretion in humans[J]. Cardiovasc Res, 2010, 87(4): 769-777. doi: 10.1093/cvr/cvq104
[11] Tsivgoulis G, Katsanos AH, Sandset EC, et al. Thrombolysis for acute ischaemic stroke: current status and future perspectives[J]. Lancet Neurol. 2023, 22(5): 418-429.
[12] Saraiva M, Vieira P, O'Garra A. Biology and therapeutic potential of interleukin-10[J]. J Exp Med, 2020, 217(1): e20190418.
[13] Andersson C, Preis SR, Beiser A, et al. Associations of Circulating Growth Differentiation Factor-15 and ST2 Concentrations With Subclinical Vascular Brain Injury and Incident Stroke[J]. Stroke, 2015, 46(9): 2568-2575.
[14] Mechtouff L, Paccalet A, Crola Da Silva C, et al. Prognosis value of serum soluble ST2 level in acute ischemic stroke and STEMI patients in the era of mechanical reperfusion therapy[J]. J Neurol, 2022, 269(5): 2641-2648.
[15] Tian X, Guo Y, Wang X, et al. Serum soluble ST2 is a potential long-term prognostic biomarker for transient ischaemic attack and ischaemic stroke[J]. Eur J Neurol, 2020, 27(11): 2202-2208.
[16] Man S, Xian Y, Holmes DN, et al. Association Between Thrombolytic Door-to-Needle Time and 1-Year Mortality and Readmission in Patients With Acute Ischemic Stroke[J]. JAMA, 2020, 323(21): 2170-2184.
[17] 王耀辉, 吕喆, 金雷雷, 等. 急性脑梗死重组组织型纤溶酶原激活剂溶栓治疗出血转化的危险因素分析[J]. 临床急诊杂志, 2020, 21(5): 380-384. https://www.cnki.com.cn/Article/CJFDTOTAL-ZZLC202005010.htm
[18] Liu C, Xie J, Sun S, et al. Hemorrhagic Transformation After Tissue Plasminogen Activator Treatment in Acute Ischemic Stroke[J]. Cell Mol Neurobiol, 2022, 42(3): 621-646.
[19] Liu H, Hu W, Zhang F, et al. Efficacy and safety of rt-PA intravenous thrombolysis in patients with wake-up stroke: A meta-analysis[J]. Medicine(Baltimore), 2022, 101(7): e28914.
[20] Bevers MB, Booraem C, Li K, et al. Association of Soluble ST2 With Functional Outcome, Perihematomal Edema, and Immune Response After Intraparenchymal Hemorrhage[J]. Neurology, 2023, 100(13): e1329-e1338.
[21] Chen J, Xiao P, Song D, et al. Growth stimulation expressed gene 2(ST2): Clinical research and application in the cardiovascular related diseases[J]. Front Cardiovasc Med, 2022, 9(1): 1007450.
-
图(2)
表(2)
计量
- 文章访问数: 414
- PDF下载数: 274
- 施引文献: 0