
Predictive value of CD63 and antithrombin-Ⅲ for secondary multiple organ dysfunction syndrome in sepsis patients
-
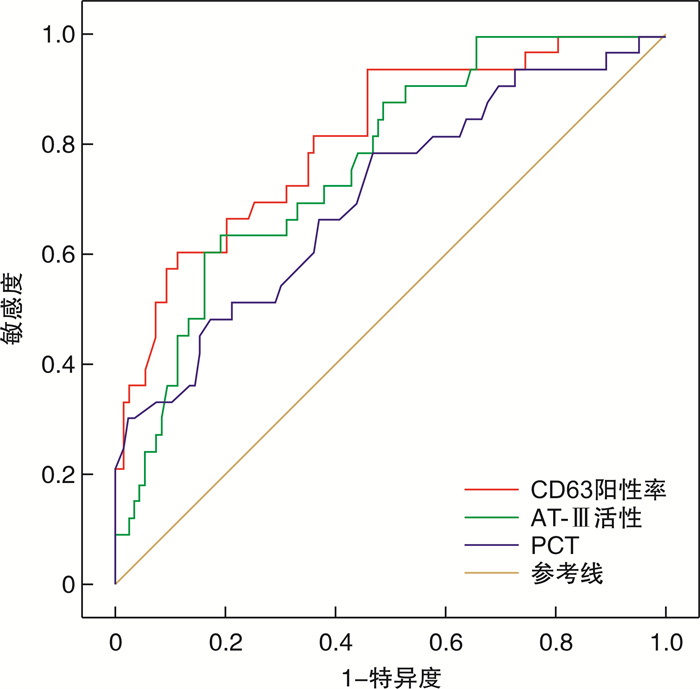
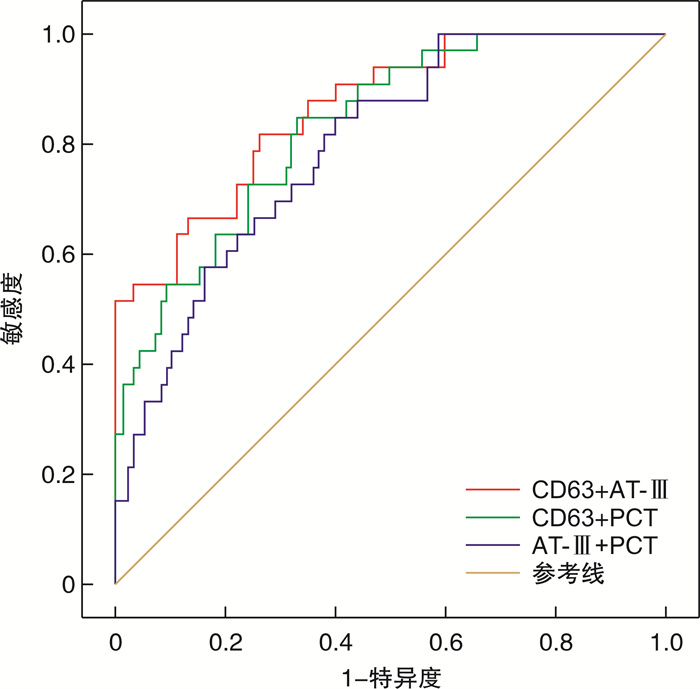
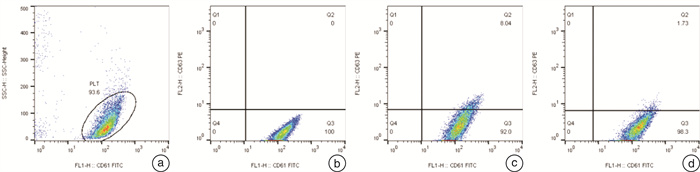
摘要: 目的 通过研究脓毒症继发多器官功能障碍综合征(MODS)患者血小板CD63与抗凝血酶-Ⅲ(AT-Ⅲ)表达水平的变化,探讨其对病情转归的预测价值。方法 选取2017年2月-2021年2月期间昆山市第一人民医院急诊科和昆山市中西医结合医院重症医学科收治的142例脓毒症患者,根据7 d内是否继发MODS分为MODS组(107例)和非MODS组(35例)。分别于入院24 h内和第3天抽取血标本,用流式细胞仪检测患者CD63阳性表达率和平均荧光强度。检测患者入院后同时间段血常规、抗凝血酶-Ⅲ(AT-Ⅲ)、降钙素原(PCT)、C反应蛋白(CRP)、血乳酸、D-二聚体、活化部分凝血活酶时间(APTT)、凝血酶原时间(PT)等。研究各数据之间的相关性采用Pearson分析,对差异有统计学意义的变量进行二元logistic回归分析,以确定脓毒症患者继发MODS的独立危险因素。采用受试者工作特征曲线(ROC曲线)分析血小板CD63联合AT-Ⅲ对脓毒症患者继发MODS的预测价值。结果 与非MODS组相比,MODS组的CD63表达水平显著增高[(9.35±0.93)% vs.(5.12±1.17)%,P< 0.01],而AT-Ⅲ活性则显著降低(70.05±4.51 vs.89.16±6.80,P< 0.01)。二元logistic回归分析显示:CD63[OR=1.304,P< 0.01]、AT-Ⅲ活性(OR=0.964,P< 0.01)和PCT(OR=1.024,P< 0.05)是影响脓毒症患者继发MODS的独立危险因素。通过分析ROC曲线发现,CD63及AT-Ⅲ对脓毒症继发MODS的预测价值均较高(AUC分别为0.8177、0.7714)。CD63联合AT-Ⅲ对于脓毒症继发MODS可能具有更好的预测能力(AUC=0.8665,敏感度为81.82%,特异度为74.26%)。结论 在一定程度上,早期检测CD63、AT-Ⅲ的水平可以用于预测脓毒症患者继发MODS的风险。
-
关键词:
- 脓毒症 /
- 多器官功能障碍综合征 /
- CD63 /
- 抗凝血酶-Ⅲ /
- 流式细胞术
Abstract: Objective To investigate the expression of Platelet CD63 and antithrombin-Ⅲ(AT-Ⅲ) in patients with sepsis-induced multiple organ dysfunction syndrome(MODS), and to explore the predictive value for disease outcome.Methods We adopted 142 ICU patients with sepsis from Feb. 2017 to Feb. 2021, and divided them into MODS group(107 cases) and non-MODS group(35 cases) according to whether secondary MODS occurred within 7 days. Blood samples were collected on the first day and the third day after admission for analysis of CD63 positive expression rate and average fluorescence intensity by flow cytometry. Blood routine, AT-Ⅲ, PCT, CRP, serum lactate acid, D-dimers, APTT, PT, et al. were detected at the same time after admission in two groups. Clinical and laboratory data between the two groups were analyzed, and the correlation between the data was analyzed by Pearson. Binary logistic regression was performed on variables with statistically significant differences to determine independent risk factors for sepsis-induced MODS patients. Finally, the positive predictive value of platelet CD63 combined with AT-Ⅲ on secondary MODS in patients with sepsis was assessed by using ROC curve.Results Compared with non-MODS group, the expression level of CD63 in MODS group was significantly increased[(9.35±0.93)% vs. (5.12±1.17)%,P< 0.01], while the activity of AT-Ⅲ was significantly decreased(70.05±4.51 vs. 89.16±6.80,P< 0.01). Binary logistic regression analysis showed that CD63(OR=1.304,P< 0.01), AT-Ⅲ activity(OR=0.964,P< 0.01) and PCT(OR=1.024,P< 0.05) were independent risk factors for sepsis-induced MODS. The analysis of ROC curve showed that CD63 and AT-Ⅲ had high predictive value for the secondary MODS of sepsis(AUC was 0.8177 and 0.7714 respectively). The combined detection of CD63 with AT-Ⅲ may have a higher predictive value for sepsis-induced MODS(AUC=0.8665, sensitivity 81.82%, specificity 74.26%).Conclusion Early detection of CD63 and AT-Ⅲ is conductive to predict the risk of secondary MODS in sepsis patients.-
Key words:
- sepsis /
- multiple organ dysfunction syndrome /
- CD63 /
- antithrombin-Ⅲ /
- flow cytometry
-

-
表 1 MODS组与非MODS组的比较
X±S 指标 MODS组 非MODS组 t/χ2/z P 性别/例 0.279 0.78 男 64 20 女 43 15 年龄/岁 61.8± 3.3 53.9± 6.8 2.266 0.025 HR/(次·min-1) 111.47± 29.36 109.83± 31.21 0.991 0.293 体温/℃ 37.61± 0.57 37.75± 0.61 -1.387 0.304 呼吸频率/(次·min-1) 17.85± 5.13 17.98± 4.73 -0.716 0.641 氧合指数/mmHg 267.45± 23.31 226.18± 20.73 13.309 0.001 吸烟史/例 0.253 0.381 有 59 21 无 48 14 酗酒史/例 0.430 0.331 有 37 10 无 70 25 CD63阳性率/% 9.35± 0.93 5.12±1.17 4.639 0 血小板计数/(×109·L-1) 147.2 ± 14.80 195± 29.6 3.057 0.003 白细胞计数/(×109·L-1) 15.36± 1.99 13.34 ± 2.14 1.387 0.169 PCT/(ng·mL-1) 37.01± 7.62 13.52± 8.31 3.259 0.001 CRP/(mg·dL-1) 20.79±3.03 15.37±4.55 1.829 0.070 乳酸/(mmol·L-1) 4.20±0.62 2.52±0.73 3.599 0 D-二聚体/(mg·L-1 FEU) 11.53±2.88 8.73±3.56 1.234 0.221 AT-Ⅲ活性/% 70.05±4.51 89.16±6.80 4.151 0 APTT/s 41.84± 3.26 35.62 ± 4.8 1.926 0.056 PT/s 17.08± 1.63 14.56± 1.17 2.507 0.013  下载: 导出CSV
下载: 导出CSV
表 2 logistic回归分析判断脓毒症患者28 d内死亡的独立危险因素
指标 β OR 95%CI P CD63阳性率 0.266 1.304 1.139~1.493 0 PCT 0.024 1.024 1.006~1.043 0.010 AT-Ⅲ活性 -0.037 0.964 0.939~0.989 0.005 常量 1.730 5.642 - 0.140
下载: 导出CSV
表 3 CD63、AT-Ⅲ和PCT对脓毒症患者继发MODS的预测能力
指标 AUC 95%CI P 截断值 敏感度/% 特异度/% CD63阳性率 0.8177 0.7339~0.9015 0 4.21 60.61 89.11 AT-Ⅲ 0.7714 0.6848~0.8579 0 87.6 63.64 81.19 PCT 0.7108 0.6053~0.8162 0 15.05 78.79 53.47
下载: 导出CSV
表 4 3种预测因子对脓毒症继发MODS的联合预测能力
指标 AUC 95%CI P 敏感度/% 特异度/% CD63联合AT-Ⅲ 0.8665 0.7974~0.9356 0 81.82 74.26 CD63联合PCT 0.8347 0.7602~0.9091 0 84.85 67.33 AT-Ⅲ联合PCT 0.7981 0.7180~0.8782 0 84.85 60.40
下载: 导出CSV
-
[1] Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3)[J]. JAMA, 2016, 315(8): 801-810. doi: 10.1001/jama.2016.0287
[2] 许涛, 盛晓华, 崔勇平, 等. CRRT在脓毒血症急性肾损伤患者救治中的临床研究[J]. 中国血液净化, 2013, 12(11): 646-650. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGJH201312003.htm
[3] 王玉, 韩艺, 周苏明. 平均血小板体积对老年脓毒症继发MODS病人病情转归的预测价值[J]. 实用老年医学, 2017, 31(6): 532-535. https://www.cnki.com.cn/Article/CJFDTOTAL-SYLA201706010.htm
[4] 许燕京, 朱然, 孙旖旎, 等. 抗凝血酶-Ⅲ对脓毒症DIC的早期诊断价值: 附445例患者的回顾性分析[J]. 中华危重病急救医学, 2017, 29(2): 127-132. doi: 10.3760/cma.j.issn.2095-4352.2017.02.007
[5] 陈伟, 胡志华, 陈勉. 脓毒症患者血浆中抗AT Ⅲ水平测定的临床意义[J]. 海南医学院学报, 2015, 21(8): 1060-1065. https://www.cnki.com.cn/Article/CJFDTOTAL-HNYY201508016.htm
[6] Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 update[J]. Intensive Care Med, 2018, 44(6): 925-928. doi: 10.1007/s00134-018-5085-0
[7] Thomas MR, Storey RF. The role of platelets in inflammation[J]. Thromb Haemost, 2015, 114(3): 449-458.
[8] 陶涛, 刘龙, 陈阳, 等. 早期检测脓毒症患者血小板CD63 CD42b CD36表达的临床意义[J]. 中国急救医学, 2020, 40(1): 58-64. doi: 10.3969/j.issn.1002-1949.2020.01.012
[9] Kasahara E, Inoue M. Cross-talk between HPA-axis-increased glucocorticoids and mitochondrial stress determines immune responses and clinical manifestations of patients with sepsis[J]. Redox Rep, 2015, 20(1): 1-10. doi: 10.1179/1351000214Y.0000000107
[10] 黄业, 易文枫, 黄贵. 脓毒症患者凝血功能指标与预后的关系[J]. 临床医学研究与实践, 2020, 5(23): 115-116. https://www.cnki.com.cn/Article/CJFDTOTAL-YLYS202023045.htm
[11] 中国中西医结合学会急救医学专业委员会. 重修"95庐山会议"多器官功能障碍综合征病情分期诊断及严重程度评分标准(2015)[J]. 中华危重病急救医学, 2016, 28(2): 99-101. doi: 10.3760/cma.j.issn.2095-4352.2016.02.002
[12] Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock(Sepsis-3)[J]. JAMA, 2016, 315(8): 801-810. doi: 10.1001/jama.2016.0287
[13] Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016[J]. Crit Care Med, 2017, 45(3): 486-552. doi: 10.1097/CCM.0000000000002255
[14] 万婷, 张小彬, 杨晓军. 平均血小板体积和血小板计数对脓毒症患者发生MODS的预测价值[J]. 国际检验医学杂志, 2020, 41(22): 2705-2708. doi: 10.3969/j.issn.1673-4130.2020.22.005
[15] 董世笑. 抗凝血酶Ⅲ、蛋白C水平与脓毒症患者病情严重程度及预后关系的临床研究[J]. 中国现代医生, 2020, 58(32): 114-117. https://www.cnki.com.cn/Article/CJFDTOTAL-ZDYS202032030.htm
[16] 万婷, 张小彬, 杨晓军. 平均血小板体积和血小板计数对脓毒症患者发生MODS的预测价值[J]. 国际检验医学杂志, 2020, 41(22): 2705-2708. doi: 10.3969/j.issn.1673-4130.2020.22.005
[17] 郑印, 郭小丹, 张正阳. 血小板参数与老年脓毒症病情严重程度的关系及对短期预后的预测作用[J]. 临床急诊杂志, 2020, 21(4): 271-276, 281. http://zzlc.cbpt.cnki.net/WKC/WebPublication/paperDigest.aspx?paperID=ea34b6de-9d32-43f4-a292-2bdcc2f67395
[18] 包晓婧, 冯若飞, 马忠仁. CD63分子的研究进展[J]. 西北民族大学学报(自然科学版), 2015, 36(3): 22-26. doi: 10.3969/j.issn.1009-2102.2015.03.006
[19] Marck RE, van der Bijl I, Korsten H, et al. Activation, function and content of platelets in burn patients[J]. Platelets, 2019, 30(3): 396-402. doi: 10.1080/09537104.2018.1448379
[20] Silverstein RL. Inflammation, atherosclerosis, and arterial thrombosis: role of the scavenger receptor CD36[J]. Cleveland Clin J Med, 2009, 76(Suppl 2): S27-30.
[21] Allingstrup M, Wetterslev J, Ravn FB, et al. Antithrombin Ⅲ for critically ill patients: a systematic review with meta-analysis and trial sequential analysis[J]. Intensive Care Med, 2016, 42(4): 505-520. doi: 10.1007/s00134-016-4225-7
[22] Karon BS, Tolan NV, Wockenfus AM, et al. Evaluation of lactate, white blood cell count, neutrophil count, procalcitonin and immature granulocyte count as biomarkers for sepsis in emergency department patients[J]. Clin Biochem, 2017, 50(16-17): 956-958. doi: 10.1016/j.clinbiochem.2017.05.014
-
图(3)
表(4)
计量
- 文章访问数: 1245
- PDF下载数: 568
- 施引文献: 0