
Predictive value of modified HEART score for the extent of coronary artery lesions in patients with moderate to low-risk suspected NSTE-ACS
-
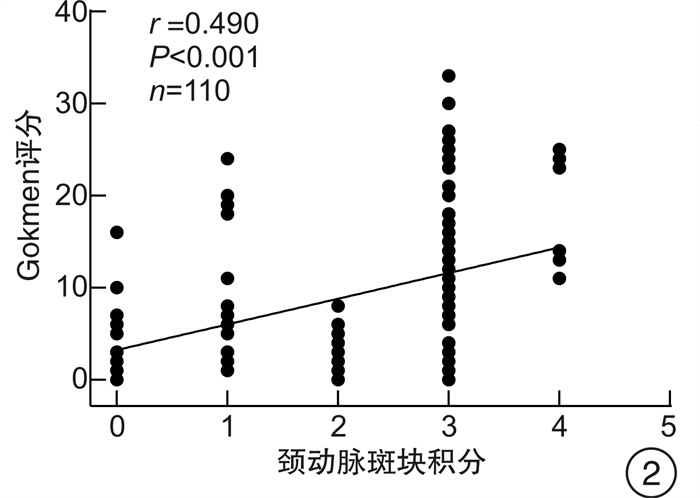
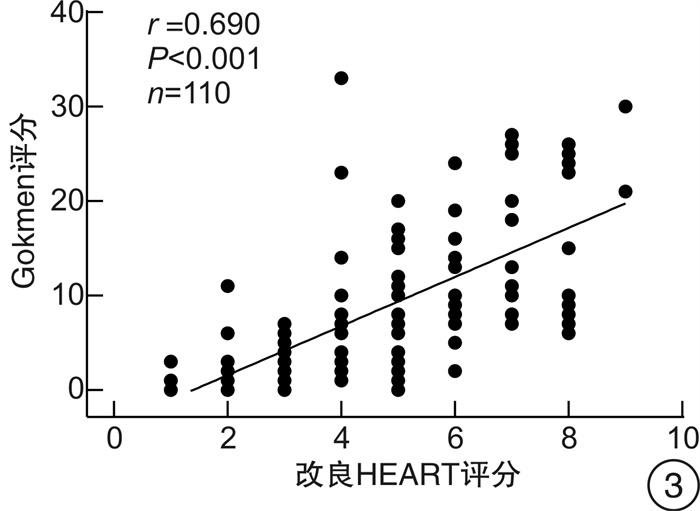
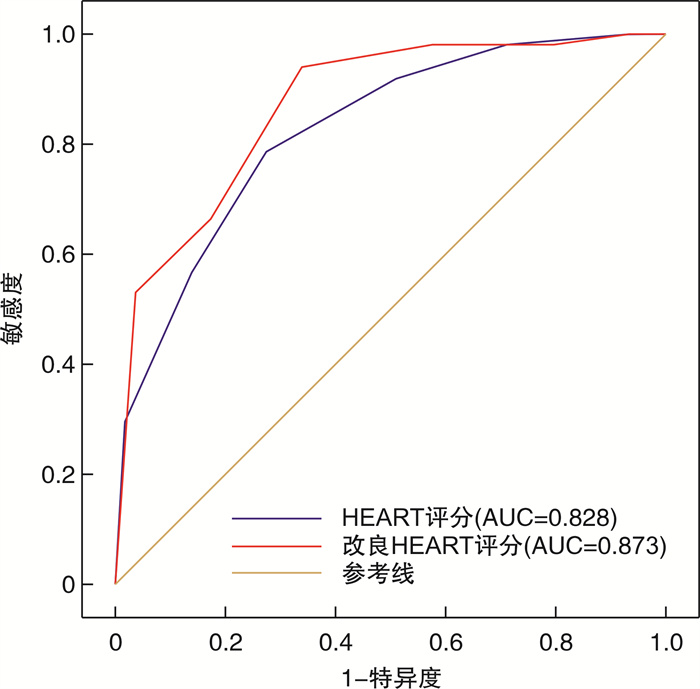
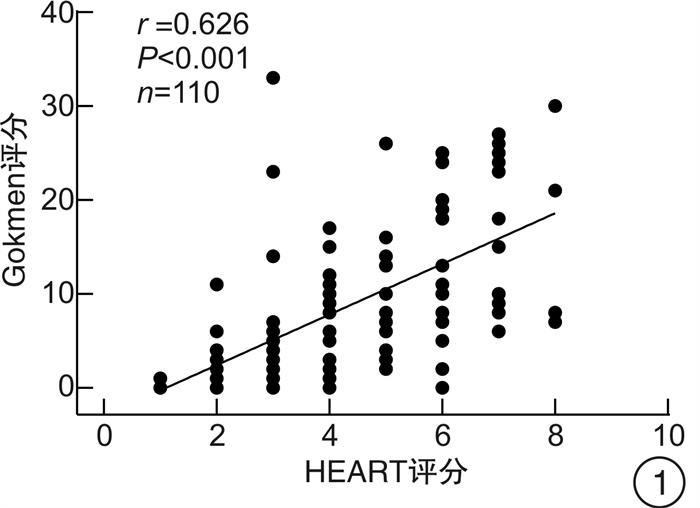
摘要: 目的 探讨改良HEART评分对中低危可疑NSTE-ACS患者冠状动脉病变程度的预测价值。方法 连续选取2020年1月—2020年12月期间在中国科学技术大学附属第一医院急救医学中心就诊的中低危可疑NSTE-ACS患者110例,收集所有患者的病史、年龄、危险因素、超敏肌钙蛋白、心电图结果以及颈动脉彩超等资料,并对所有患者进行HEART评分和改良HEART评分。根据改良HEART评分结果把研究对象分为3组:低危组29例,中危组55例,高危组26例,比较各组间一般临床资料、冠状动脉造影Gokmen评分、颈动脉斑块积分的差异; Gokmen评分 < 7分为轻度冠状动脉病变,采用ROC曲线比较两种评分预测轻度冠状动脉病变患者的效能。结果 随着改良HEART评分危险分层上升,患者颈动脉斑块积分、Gokmen评分增加(P< 0.05);Spearman相关分析结果显示,HEART评分与冠状动脉Gokmen评分呈正相关(r=0.626,P< 0.01),颈动脉斑块积分与冠状动脉Gokmen评分呈正相关(r=0.490,P< 0.01),改良HEART评分与冠状动脉Gokmen评分呈正相关(r=0.690,P< 0.01);改良HEART评分预测轻度冠状动脉病变患者的ROC曲线下面积为0.873(95%CI:0.796~0.929),HEART评分的ROC曲线下面积为0.828(95%CI:0.744~0.893),改良HEART评分预测轻度冠状动脉病变的ROC曲线下面积、敏感度高于HEART评分,差异有统计学意义(P< 0.05)。结论 改良HEART评分预测中低危可疑NSTE-ACS患者冠状动脉病变程度的能力优于HEART评分。Abstract: Objective To investigate the predictive value of the modified HEART score on the extent of coronary artery lesions in patients with low-and medium-risk suspected NSTE-ACS.Methods One hundred and ten consecutive suspected NSTE-ACS patients with moderate to low risk were enrolled from the department of emergency medicine of the First Affiliated Hospital of USTC from January to December in 2020 were enrolled, and the medical history, age, risk factors, troponin, electrocardiographic findings and carotid ultrasound were collected from all patients, and the HEART score and modified HEART score. The study subjects were divided into three groups according to the modified HEART score: low-risk group(n=29), intermediate-risk group(n=55), and high-risk group(n=26), and the differences in general clinical information, coronary angiography Gokmen score, and carotid plaque score were compared between the groups; Gokmen score < 7 was classified as mild coronary artery lesion, and the ROC curve was used to analyze the two scores to predict the effectiveness of mild The ROC curve was used to predict the efficacy of the two scores in patients with mild coronary artery lesions.Results The carotid plaque score and Gokmen score increased with the risk stratification of the modified HEART score (P< 0.05).Spearman's correlation analysis showed that HEART score was positively correlated with coronary Gokmen score(r=0.626,P< 0.01), carotid plaque score was positively correlated with coronary Gokmen score(r=0.490,P< 0.01), and the modified HEART score was positively correlated with the coronary Gokmen score(r=0.690,P< 0.01); the area under the ROC curve of the modified HEART score predicted 0.873(95%CI: 0.796-0.929) in patients with mild coronary artery lesions, and the area under the ROC curve for the HEART score The area under the ROC curve of the HEART score was 0.828(95%CI: 0.744-0.893), and the area under the ROC curve of the HEART score was higher than that of the HEART score in predicting mild coronary artery lesions(P< 0.05).Conclusion The modified HEART score was superior to the HEART score in predicting the extent of coronary artery lesions in patients with moderate to low-risk suspected NSTE-ACS.
-
Key words:
- HEART score /
- carotid plaque score /
- coronary artery lesion /
- prediction
-

-
表 1 HEART评分及改良HEART评分方法
项目 HEART评分 得分 改良HEART评分 得分 病史 高度可疑
中度可疑
轻度可疑2
1
0中、高度可疑
轻度可疑1
0心电图 典型ST段抬高
非特异性复极异常,束支传导阻滞,左室肥厚
正常2
1
0非特异性复极异常,束支传导阻滞,左室肥厚
正常1
0年龄/岁 >65
45~65
< 452
1
0>65
≤651
0危险因素/个 ≥3
1~2
02
1
0≥3
1~2
02
1
0肌钙蛋白 >2倍标准值
标准值1~2倍
< 标准值2
1
0>2倍标准值
标准值1~2倍
< 标准值2
1
0颈动脉斑块积分 5分
3~4分
1~2分
0分3
2
1
0注:危险因素包括高血压、糖尿病、高脂血症、肥胖、吸烟、冠心病家族史。  下载: 导出CSV
下载: 导出CSV
表 2 不同组冠状动脉Gokmen评分和颈动脉斑块积分比较
项目 低危组(29例) 中危组(55例) 高危组(26例) Gokmen评分 2.00(1.00,4.00) 7.50(3.00,13.25)1) 18.00(9.75,25.00)1)2) 颈动脉斑块积分 1.00(0.00,2.00) 3.00(2.00,3.00)1) 3.00(3.00,3.00)1)2) 与低危组比较,1)P < 0.05;与中危组比较,2)P < 0.05。
下载: 导出CSV
表 3 两种评分预测轻度冠脉病变的效能比较
评分 截点值 敏感度 特异度 准确度 假阴性率 假阳性率 阳性预测值 阴性预测值 HEART评分 4.90 0.784 (40/51) 0.729 (43/59) 0.755 (83/110) 0.216 (11/51) 0.271 (16/59) 0.714 (40/56) 0.796 (43/54) 改良HEART评分 5.10 0.941 (48/51) 0.661 (39/59) 0.791 (87/110) 0.059 (3/51) 0.339 (20/59) 0.706 (48/68) 0.929 (39/42) χ2 5.299 0.640 0.414 5.299 0.640 0.011 2.156 P 0.021 0.424 0.520 0.021 0.424 0.918 0.142
下载: 导出CSV
-
[1] 薛军, 韩占红, 王明晓, 等. 北京市急诊胸痛的病因学调查分析[J]. 中国综合临床, 2012, 33(10): 1042-1046. doi: 10.3760/cma.j.issn.1008-6315.2012.10.011
[2] 中华心血管病杂志编辑委员会, 胸痛规范化评估与诊断共识专家组. 胸痛规范化评估与诊断中国专家共识[J]. 中华心血管病杂志, 2014, 42(8): 627-632. doi: 10.3760/cma.j.issn.0253-3758.2014.08.002
[3] Foy AJ, Liu G, Davidson WR, Jr., et al. Comparative effectiveness of diagnostic testing strategies in emergency department patients with chest pain: an analysis of downstream testing, interventions, and outcomes[J]. JAMA Intern Med, 2015, 175(3): 428-436. doi: 10.1001/jamainternmed.2014.7657
[4] Mookadam F, Tanasunont W, Jalal U, et al. Carotid intima-media thickness and cardiovascular risk[J]. Future Cardiol, 2011, 7(2): 173-182. doi: 10.2217/fca.11.2
[5] 康爽. 彩色多普勒超声诊断脑梗死患者颈动脉粥样硬化斑块的价值研究[J]. 影像研究与医学应用, 2020, 4(16): 151-152. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYY202016107.htm
[6] Rahko PS. Rapid evaluation of chest pain in the emergency department[J]. JAMA Intern Med, 2014, 174(1): 59-60. doi: 10.1001/jamainternmed.2013.9978
[7] Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation[J]. Eur Heart J, 2021, 42(14): 1289-1367. doi: 10.1093/eurheartj/ehaa575
[8] Cosmi D, Mariottoni B, Cosmi F. Stable atypical chest pain with negative anatomical or functional diagnostic test: Diagnosis no matter what or prevention at any cost?[J]. Clin Cardiol, 2019, 42(10): 982-987. doi: 10.1002/clc.23250
[9] Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines[J]. Circulation, 2014, 130(25): e344-426.
[10] Backus BE, Six AJ, Kelder JH, et al. Risk scores for patients with chest pain: evaluation in the emergency department[J]. Curr Cardiol Rev, 2011, 7(1): 2-8. doi: 10.2174/157340311795677662
[11] Long B, Koyfman A. Best Clinical Practice: Current Controversies in the Evaluation of Low-Risk Chest Pain with Risk Stratification Aids. Part 2[J]. J Emerg Med, 2017, 52(1): 43-51. doi: 10.1016/j.jemermed.2016.07.004
[12] Mahler SA, Riley RF, Hiestand BC, et al. The HEART Pathway randomized trial: identifying emergency department patients with acute chest pain for early discharge[J]. Circ Cardiovasc Qual Outcomes, 2015, 8(2): 195-203. doi: 10.1161/CIRCOUTCOMES.114.001384
[13] 高瑛子, 高传玉. 颈动脉硬化与冠心病的相关性[J]. 中国动脉硬化杂志, 2015, 23(9): 942-944. https://www.cnki.com.cn/Article/CJFDTOTAL-KDYZ201509019.htm
[14] Jashari F, Ibrahimi P, Nicoll R, et al. Coronary and carotid atherosclerosis: similarities and differences[J]. Atherosclerosis, 2013, 227(2): 193-200. doi: 10.1016/j.atherosclerosis.2012.11.008
[15] Amato M, Veglia F, de Faire U, et al. Carotid plaque-thickness and common carotid IMT show additive value in cardiovascular risk prediction and reclassification[J]. Atherosclerosis, 2017, 263: 412-419. doi: 10.1016/j.atherosclerosis.2017.05.023
[16] 宋昌鹏, 王德昭, 胡宏宇等. 高分辨率磁共振评价冠状动脉粥样硬化患者的颈动脉斑块特征[J]. 中华心血管病杂志, 2016, 44(1): 38-42. doi: 10.3760/cma.j.issn.0253-3758.2016.01.009
[17] 任静, 翁萍, 吐尔逊纳依·纳孜尔等. 颈动脉斑块积分对冠状动脉病变的预测价值[J]. 中国循环杂志, 2017, 32(9): 882-885. doi: 10.3969/j.issn.1000-3614.2017.09.012
[18] Yur'eva EA, Sukhorukov VS, Murashov AN, et al. Biochemical indicators of atherogenic and protective activity of xydiphone in experimental animals[J]. Bull Exp Biol Med, 2012, 153(4): 459-462. doi: 10.1007/s10517-012-1740-6
-
图(4)
表(3)
计量
- 文章访问数: 1008
- PDF下载数: 252
- 施引文献: 0