
Trends in clinical outcomes and survival following prehospital thrombolytic therapy given by ambulance clinicians for acute ST elevation myocardial infarction in Changde rural areas
-
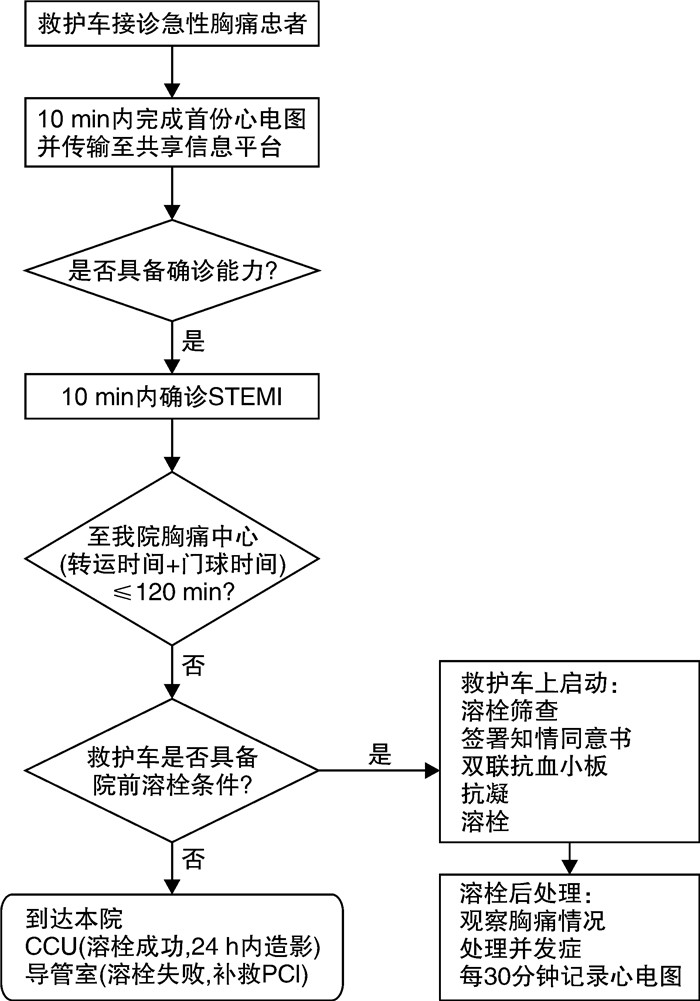
摘要: 目的 探索常德农村地区急性ST段抬高型心肌梗死(ST-segment elevation myocardial infarction,STEMI)患者院前溶栓治疗后的临床结局和生存趋势。方法 观察2020-2022年常德农村地区给予院前溶栓患者的临床结局。院前医生接诊可疑心肌梗死的患者后,对其进行初步的评估与治疗,评估包括完善床旁12导心电图、肌钙蛋白T,心电图通过远程心电系统,将信息传输给院内胸痛中心(急诊科、心内科、导管室),肌钙蛋白T的结果通过院内胸痛中心微信群进行传输,患者的基本信息、体检结果以及相关临床指标通过院前电子病历系统,实施院前与胸痛中心的互通。是否行溶栓治疗由心内科专家进行决策。结果 共385例STEMI患者接受院前溶栓治疗,患者年龄中位数为61.2岁,其中77%为男性,院前再灌注治疗节省的时间为131 min。在症状出现后2 h内接受院前溶栓治疗的比例从2020年的21%上升到2022年的39%,差异有统计学意义(P=0.003)。首次医疗接触后24 h内接受冠状动脉造影或经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)的患者比例从56.4%增加到95.6%,差异有统计学意义(P < 0.001)。STEMI后收缩期心力衰竭从19.3%下降到8.9%,差异有统计学意义(P=0.021),而患者1年死亡率下降了50%,达到5.6%。13例患者出现急性院外心脏骤停(out-of-hospital cardiac arrest,OHCA),所有患者均成功除颤。10例(2.6%)患者发生重大出血事件。结论 院前溶栓治疗是一种可行和安全的干预措施,可用于STEMI长距离转诊过程中,PCI实施前改善心肌再灌注的先行方案。
-
关键词:
- ST段抬高型心肌梗死 /
- 溶栓治疗 /
- 院前 /
- 心肌梗死 /
- 农村
Abstract: Objective To will explore the clinical outcomes and survival trends after prehospital thrombolysis in patients with acute ST elevation myocardial infarction(STEMI) in the rural area of Changde.Methods The outcomes of a prehospital thrombolytic therapy system in changde rural area during three years were observed. Electrocardiogram(ECG) through remote ECG system, the information transmission to the hospital chest pain center(emergency department, cardiology, catheterization). The results of the troponin T through the hospital chest pain center WeChat group transmission. The patient's basic information, physical examination results and related clinical indicators through pre-hospital electronic medical record system, the implementation of pre-hospital and chest pain center. The decision making whether to perform thrombolysis is made by a cardiologist.Results A total of 385 STEMI patients received prehospital thrombolytic therapy, median patient age was 61.2 years, and 77% were men. Time saved by prehospital reperfusion therapy was 131 minutes. The proportion who got prehospital thrombolytic therapy within 2 hours of symptom onset increased from 21% in 2020 to 39% in 2022, with a statistically significant difference(P=0.003). The proportion who underwent coronary angiography or percutaneous coronary intervention within 24 hours of first medical contact increased from 56.4% to 95.6%, with a statistically significant difference(P < 0.001). Post-STEMI systolic heart failure decreased from 19.3% to 8.9%, with a statistically significant difference(P=0.021), while 1-year mortality fell, non-significantly, by 50% over time to reach 5.6%. Thirteen patients suffered acute out-of-hospital cardiac arrest, all were successfully defibrillated. Ten patients had major bleeding events(2.6%).Conclusion Prehospital thrombolytic therapy is a feasible and safe intervention used in rural settings with long evacuation lines before percutaneous coronary intervention facilities. -

-
表 1 2020-2022年STEMI患者接受PHT治疗的基本资料
变量 2020-2022(385例) 2020(140例) 2021(155例) 2022(90例) P 基本资料 年龄(IQR)/岁 61.2(53.2,69.8) 61.9(53.1,71.3) 60.7(53.4,69.8) 61.4(53.4,67.7) 0.611 男性/例(%) 295(77) 106(76) 116(75) 73(81) 0.401 时间延迟 症状发生到完成心电图(IQR) 110(65,170) 113(84,175) 103(57,161) 108(62,165) 0.121 院前完成心电图到PHT (IQR) 36(25,53) 34(26,50) 37(25,55) 36(23,53) 0.721 症状发生到PHT(IQR) 150(108,211) 155(124,210) 143(105,207) 146(93,218) 0.071 症状发生到PHT < 2 h/ 例(%) 116(30.1) 29(21.0) 52(33.5) 35(39.0) 0.003 FMC至冠脉造影(IQR)/h 7.4(3.3,21.1) 23.7(4.1,53.2) 5.7(3.1,14.2) 4.3(2.9,14.3) < 0.001 FMC至冠脉造影 < 24 h/例(%) 307(79.4) 79(56.4) 142(91.5) 86(95.6) < 0.001 侵入性操作/例(%) 冠脉造影 338(87.8) 103(73.6) 146(94.2) 89(98.9) < 0.001 PCI 266(69.1) 84(60.0) 112(72.3) 70(77.8) 0.003 冠脉搭桥 38(9.9) 6(4.3) 19(12.3) 13(14.4) 0.011  下载: 导出CSV
下载: 导出CSV
表 2 2020—2022年接受PHT治疗患者的左心室功能、肌钙蛋白水平和病死率
变量 2020—2022(385例) 2020(140例) 2021(155例) 2022(90例) P LVEF < 40%/例(%) 50(13.0) 27(19.3) 15(9.8) 8(8.9) 0.021 1年病死/例(%) 31(8.1) 16(11.4) 10(6.5) 5(5.6) 0.092 肌钙蛋白T峰值(IQR)/(ng/mL) 6.1(2.8,10.8) 7.3(3.7,12.9) 5.8(2.7,10.3) 5.0(2.1,9.2) 0.031
下载: 导出CSV
表 3 STEMI患者症状发生到PHT开始与临床结局的关系
变量 症状开始到PHT时间/min P < 120(122例) 120~239(158例) ≥240(105例) 基本资料 年龄(IQR)/岁 59.0(50.9,67.7) 61.6(53.4,70.3) 63.3(56.0,72.0) 0.311 男性/例(%) 93(76.2) 125(79.1) 77(73.3) 0.121 结局/例(%) 收缩期心衰 9(7.3) 23(14.6) 18(17.1) 0.002 1年病死率 4(3.3) 15(9.50) 12(11.4) 0.011
下载: 导出CSV
-
[1] Liu X, Huang S, Cheng J, et al. Application Effect of Intelligent Monitoring of Emergency Nursing Process Reengineering in the Thrombolytic Therapy of Acute Myocardial Infarction[J]. Contrast Media Mol Imaging, 2021, 2021: 3043289.
[2] Dauerman HL, Ibanez B. The Edge of Time in Acute Myocardial Infarction[J]. J Am Coll Cardiol, 2021, 77(15): 1871-1874. doi: 10.1016/j.jacc.2021.03.003
[3] Murphy A, Goldberg S. Mechanical Complications of Myocardial Infarction[J]. Am J Med, 2022, 135(12): 1401-1409. doi: 10.1016/j.amjmed.2022.08.017
[4] Aoun J, Kleiman NS, Goel SS. Diagnosis and Management of Late-presentation ST-elevation Myocardial Infarction and Complications[J]. Interv Cardiol Clin, 2021, 10(3): 369-380.
[5] Kiefer JJ, Augoustides JG. Acute Myocardial Infarction With Cardiogenic Shock: -Navigating the Invasive Options in Clinical Management[J]. J Cardiothorac Vasc Anesth, 2021, 35(11): 3154-3157. doi: 10.1053/j.jvca.2021.07.014
[6] Almeida I, Miranda H, Santos H, et al. Cocaine-associated myocardial infarction: Features of diagnosis and treatment[J]. J Electrocardiol, 2021, 67(1): 11-12.
[7] 颜红兵, 向定成, 刘红梅, 等. ST段抬高型急性心肌梗死院前溶栓治疗中国专家共识[J]. 中国医学前沿杂志(电子版), 2018, 10(4): 1-10. https://www.cnki.com.cn/Article/CJFDTOTAL-YXQY201804001.htm
[8] 夏海云, 丁霞, 傅琳. 现场快速检测高敏肌钙蛋白在老年急性心肌梗死早期的临床诊断价值[J]. 临床急诊杂志, 2022, 23(1): 67-71. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.01.015
[9] 唐茜, 王玉, 程景林. 替罗非班联合呋塞米对急性心肌梗死伴心力衰竭患者行急诊PCI后临床预后的影响[J]. 临床急诊杂志, 2022, 22(7): 441-444. doi: 10.13201/j.issn.1009-5918.2021.07.001
[10] Thygesen K, Jaffe AS. Adjusting the MI Codes Into the Framework of the Universal Definition of Myocardial Infarction[J]. J Am Coll Cardiol, 2021, 77(7): 858-860. doi: 10.1016/j.jacc.2021.01.003
[11] Khalil M, Ahmed MT, Alabdallah K, et al. Double Trouble: Acute Myocardial Infarction Caused by Thrombosis of a Coronary Cameral Fistula From Anomalous Right Coronary Artery[J]. Cardiovasc Revasc Med, 2022, 34: 152-153. doi: 10.1016/j.carrev.2021.08.015
[12] Oh S, Hyun DY, Cho KH, et al. Long-term outcomes in ST-elevation myocardial infarction patients treated according to hospital visit time[J]. Korean J Intern Med, 2022, 37(3): 605-617. doi: 10.3904/kjim.2021.204
[13] Bhatt DL, Lopes RD, Harrington RA. Diagnosis and Treatment of Acute Coronary Syndromes: A Review[J]. JAMA, 2022, 327(7): 662-675. doi: 10.1001/jama.2022.0358
[14] Berwanger O, Lopes RD, Moia D, et al. Ticagrelor Versus Clopidogrel in Patients With STEMI Treated With Fibrinolysis: TREAT Trial[J]. J Am Coll Cardiol, 2019, 73(22): 2819-2828. doi: 10.1016/j.jacc.2019.03.011
[15] Krittanawong C, Hahn J, Kayani W, et al. Fibrinolytic Therapy in Patients with Acute ST-elevation Myocardial Infarction[J]. Interv Cardiol Clin, 2021, 10(3): 381-390. http://www.sciencedirect.com/science/article/pii/S2211745821000274
[16] Hamilos M, Kanakakis J, Anastasiou I, et al. Ticagrelor versus clopidogrel in patients with STEMI treated with thrombolysis: the MIRTOS trial[J]. EuroIntervention, 2021, 16(14): 1163-1169. doi: 10.4244/EIJ-D-20-00268
[17] Fothergill RT, Watson LR, Virdi GK, et al. Survival of resuscitated cardiac arrest patients with ST-elevation myocardial infarction conveyed directly to a Heart Attack Centre by ambulance clinicians[J]. Resuscitation, 2014, 85(1): 96-98. doi: 10.1016/j.resuscitation.2013.09.010
[18] Lien Nilsen JM, Bo I, Rasmussen JR, et al. Doubled survival from out-of-hospital cardiac arrest in a rural community in North-Norway following implementation of an aggressive chest pain protocol with early prehospital thrombolysois for STEMI[J]. Circulation, 2011, 124(Suppl 21): A17087.
[19] 杲建波, 马瑞聪, 刘春蕊, 等. 全身免疫炎症指数对急性心肌梗死患者直接经皮冠状动脉介入治疗术后院内主要不良心血管事件的预测[J]. 临床急诊杂志, 2022, 23(3): 192-197. https://lcjz.whuhzzs.com/article/doi/10.13201/j.issn.1009-5918.2022.03.006
[20] Walters D, Mahmud E. Thrombolytic Therapy for ST-Elevation Myocardial Infarction Presenting to non-Percutaneous Coronary Intervention Centers During the COVID-19 Crisis[J]. Curr Cardiol Rep, 2021, 23(10): 152. doi: 10.1007/s11886-021-01576-2
[21] Bellis A, Mauro C, Barbato E, et al. The Rationale of Neprilysin Inhibition in Prevention of Myocardial Ischemia-Reperfusion Injury during ST-Elevation Myocardial Infarction[J]. Cells, 2020, 9(9): 2134. doi: 10.3390/cells9092134
[22] Govea A, Lipinksi J, Patel MP. Prehospital Evaluation, ED Management, Transfers, and Management of Inpatient STEMI[J]. Interv Cardiol Clin, 2021, 10(3): 293-306.
[23] Marcolino MS, Ribeiro AL. Focusing on prehospital care to improve ST elevation myocardial infarction care[J]. Heart, 2020, 106(5): 323-324.
[24] Van de Werf F. Reperfusion treatment in acute myocardial infarction in elderly patients[J]. Kardiol Pol, 2018, 76(5): 830-837.
[25] Welsh RC, Cantor WJ, Traboulsi M, et al. Primary Percutaneous Coronary Intervention and Application of the Pharmacoinvasive Approach Within ST-Elevation Myocardial Infarction Care Networks[J]. Can J Cardiol, 2022, 38(10 Suppl1): S5-S16.
[26] Mentias A, Girotra S. Pharmaco-Invasive Strategy: The Answer to Improving ST-Elevation-Myocardial Infarction Care[J]. J Am Heart Assoc, 2020, 9(12): e016831.
-
图(1)
表(3)
计量
- 文章访问数: 469
- PDF下载数: 73
- 施引文献: 0