
Clinical value of serum CitH3 in predicting severity and in-hospital mortality of acute pancreatitis
-
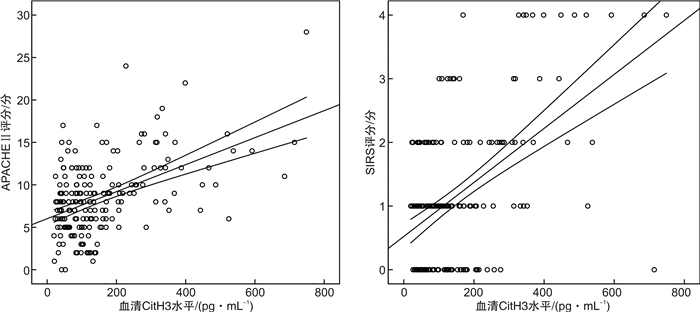
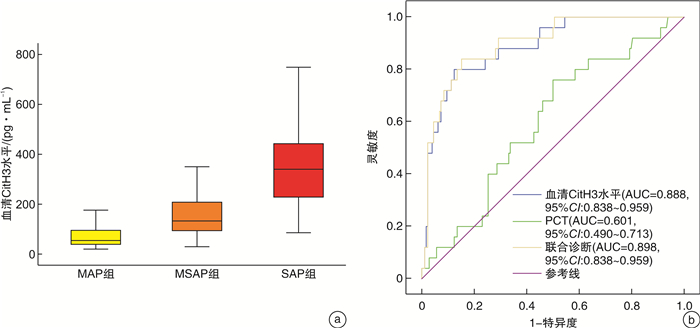
摘要: 目的 分析急性胰腺炎(AP)患者血清瓜氨酸化组蛋白H3(CitH3)与疾病严重程度及住院病死率的相关性。方法 选取2017年1月-2021年6月期间我院就诊的203例AP患者。根据2012年修订的亚特兰大急性胰腺炎分级标准将患者分为轻度AP(MAP组,84例)、中度AP(MSAP组,94例)和重度AP(SAP组,25例)。使用夹心间接酶联免疫吸附法检测血清CitH3水平。结果 SAP组患者入院时血清CitH3水平[340.00(227.00,442.50) pg/mL]显著高于MAP组[104.00(79.70,138.00) pg/mL]和MSAP组[62.40(39.60,93.40) pg/mL]患者,且MAP组与MSAP组之间比较差异有统计学意义(P<0.001)。经受试者工作特征曲线(ROC)分析,入院时血清CitH3水平联合PCT用于诊断SAP的曲线下面积(AUC)为0.898,显著优于两者单独诊断。AP患者入院时血清CitH3水平与APACHE Ⅱ评分、全身炎症反应综合征评分均呈正相关(r=0.319,0.528,P<0.001)。入院24 h时血清CitH3水平[112.40(77.50,211.50) pg/mL]较入院时基线水平[104.05(59.70,180.40) pg/mL]有所升高,差异有统计学意义(P=0.024],但入院48 h时血清CitH3水平[81.65(61.20,139.50) pg/mL]则低于入院时和入院24 h时的血清水平,差异有统计学意义(P<0.05)。经单因素和多因素logistic回归分析,入院时血清CitH3水平是影响AP患者发生住院死亡的独立危险因素(P<0.001)。经ROC曲线分析,入院时血清CitH3水平预测AP患者发生持续性器官衰竭、胰腺坏死及院内死亡的AUC分别为0.891、0.903、0.924。结论 血清CitH3水平升高与AP患者疾病进展和短期预后不良密切有关。Abstract: Objective To analyze the correlation between serum citrullination of histone 3(CitH3) and disease severity and in-hospital mortality in patients with acute pancreatitis(AP).Methods Two hundred and three AP patients in our hospital from January 2017 to June 2021 were selected. Patients were classified according to the Atlanta classification as mild AP(MAP group, n=84), moderate AP(MSAP group, n=94), and severe AP(SAP group, n=25). Serum CitH3 level was detected by sandwich indirect enzyme-linked immunosorbent assay.Results The serum CitH3 level at admission in SAP group[340.00(227.00, 442.50) pg/mL]was significantly higher than that in MAP[104.00(79.70, 138.00) pg/mL]and MSAP[62.40(39.60, 93.40) pg/mL]groups. There was also significant statistical difference between MAP and MSAP groups(P < 0.001). According to receiver operating characteristic curve(ROC) analysis, the area under curve(AUC) of serum CitH3 level at admission combined with PCT for the diagnosis of SAP at admission was 0.898, which was significantly better than that of the two factors alone. Serum CitH3 level at admission was positively correlated with APACHE Ⅱ score and systemic inflammatory response syndrome score in AP patients(r=0.319, 0.528, P < 0.001). The serum CitH3 level at 24 h after admission [112.40(77.50, 211.50) pg/mL]was slightly higher than that at admission[104.05(59.70, 180.40) pg/mL, P=0.024]. However, the serum CitH3 level at 48 h[81.65(61.20, 139.50) pg/mL]was lower than that at admission and 24 h(P < 0.05). Univariate and multivariate logistic regression analysis showed that serum CitH3 level at admission was an independent risk factor for in-hospital death in AP patients(P < 0.001). According to ROC curve analysis, serum CitH3 level at admission predicted the AUC of persistent organ failure, pancreatic necrosis and in-hospital death in AP patients were 0.891, 0.903 and 0.924, respectively.Conclusion The increase of serum CitH3 level is closely related to disease progression and poor short-term prognosis in patients with AP.
-

-
表 1 3组AP患者一般临床资料分析
例(%),X±S 指标 MAP组(84例) MSAP(94例) SAP组(25例) Z/t/χ2 P 年龄/岁 59.18±15.68 62.67±18.26 60.04±23.02 0.876 0.418 男性 48(57.14) 58(61.70) 13(52.00) 0.895 0.639 BMI 22.77±4.09 23.05±4.40 21.60±3.58 1.188 0.307 住院时间/d 9.62±5.32 16.10±7.151) 12.56±7.382) 22.210 <0.001 病因学 23.227 0.108 胆源性 41(48.81) 25(26.60) 9(36.00) 酒精性 13(15.48) 28(29.79) 4(16.00) 高甘油三酯血症 15(17.86) 19(20.21) 4(16.00) 胰管阻塞 4(4.76) 7(7.45) 3(12.00) 手术与创伤 3(3.57) 3(3.19) 1(4.0) 药源性 1(1.19) 0 0 感染及全身炎症反应 0 1(1.06) 2(8.00) 内分泌及代谢疾病 1(1.19) 1(1.06) 0 特发性 6(7.14) 10(10.64) 2(8.00) 发病至诊断时间/h 18.00(12.00,29.50) 19.00(13.50,27.50) 21.00(12.00,30.00) 1.901 0.201 Charlson合并症指数 1.00(0.00,2.00) 0.00(0.00,2.00) 0.00(0.00,2.00)1)2) 0.782 0.676 体温/℃ 36.94±0.82 36.71±0.81 37.06±0.86 2.693 0.070 HR/(次·min-1) 77.36±16.19 77.70±16.32 88.16±17.271)2) 4.615 0.011 SBP/mmHg 133.19±26.38 136.66±26.16 133.40±36.45 0.386 0.680 实验室指标 WBC/μL 9796.43±3718.51 12134.04±4833.811) 12480.00±5384.311) 7.181 0.001 PLT/(×104·L-1) 21.53±6.55 22.15±7.04 21.06±9.31 0.302 0.739 CRP/(mg·dL-1) 1.31(0.40,9.09) 0.36(0.09,1.28) 1.80(0.27,8.33) 3.791 0.150 血尿淀粉酶/(U·L-1) 1285.00 (574.00,1915.00) 1317.00 (704.00,2209.00) 1435.00 (407.00,2298.00) 2.564 0.278 LDH/(U·L-1) 303.00 (209.00,498.00) 315.00 (256.00,346.00) 329.00 (207.00,431.00) 0.816 0.665 BUN/(mg·dL-1) 19.20(16.00,23.40) 16.20(12.20,22.20) 21.00(12.50,32.30)2) 6.090 0.048 Cr/(mg·dL-1) 0.74(0.69,0.83) 0.74(0.60,0.83) 0.80(0.69,1.02) 1.488 0.475 PCT/(mg·dL-1) 0.35(0.09,2.06) 0.26(0.14,3.20) 3.25(0.78,7.16)2) 7.661 0.022 钙/(mg·dL-1) 9.11±0.45 9.11±0.69 9.02±0.67 0.247 0.781 内毒素/(U·L-1) 22.19±8.96 23.57±8.10 29.30±10.321)2) 6.378 0.002 CT表现 31.123 <0.001 胰腺低强化病变 0 32(34.04) 17(68.00) 急性胰周积液 0 77(81.91) 25(100.00) 炎症扩展至肾下极 0 31(32.98) 25(100.00) 炎症扩展至直肠膀胱陷凹 0 3(3.19) 19(76.00) APACHE Ⅱ评分/分 7.30±3.12 8.69±4.40 12.28±7.711)2) 11.920 <0.001 SIRS评分/分 1.00(1.00,2.00) 1.00(1.00,2.00)1) 3.00(2.00,3.00)1)2) 20.715 <0.001 治疗方案 63.646 <0.001 肠内营养 0 28(29.79) 25(100.00) 连续性血液透析 0 0 7(28.00) 内镜括约肌切开术 30(35.71) 21(22.34) 5(20.00) 内镜干预 0 2(2.13) 0 与MAP组比较,1)P<0.05;与MSAP组比较,2)P<0.05。  下载: 导出CSV
下载: 导出CSV
表 2 单因素和多因素logistic回归分析影响AP患者发生住院死亡的临床因素
变量 单因素分析 多因素分析 OR(95%CI) P OR(95%CI) P 年龄 0.988(0.954~1.024) 0.520 - - 性别 12.421(1.533~101.305) 0.019 28.308(1.318~607.794) 0.033 BMI 1.016(0.867~1.190) 0.845 - - 病因学 0.681(0.332~1.400) 0.297 - - 发病至诊断时间 1.009(0.997~1.021) 0.126 - - Charlson合并症指数 1.099(0.750~1.611) 0.628 - - 体温 1.361(0.640~2.893) 0.424 - - HR 1.025(0.986~1.066) 0.214 - - SBP 1.022(0.998~1.046) 0.070 - - WBC 1.000(1.000~1.001) 0.038 0.999(0.999~1.001) 0.103 PLT 1.014(0.925~1.112) 0.767 - - CRP 1.021(0.935~1.115) 0.646 - - 血尿淀粉酶 1.001(1.000~1.001) 0.004 1.001(1.000~1.001) 0.058 LDH 1.003(1.001~1.005) 0.015 1.003(1.000~1.007) 0.059 BUN 1.002(0.953~1.054) 0.944 - - Cr 0.389(0.039~3.902) 0.422 - - 血清钙 0.811(0.244~2.694) 0.733 - - 内毒素 1.019(0.620~5.019) 0.203 - - PCT 0.936(0.810~1.082) 0.371 - - APACHE Ⅱ评分 1.165(1.045~1.300) 0.006 0.836(0.673~1.039) 0.106 SIRS评分 2.491(1.333~4.654) 0.004 0.803(0.233~2.771) 0.729 入院时血清CitH3水平 1.008(1.004~1.012) <0.001 1.016(1.006~1.026) 0.002
下载: 导出CSV
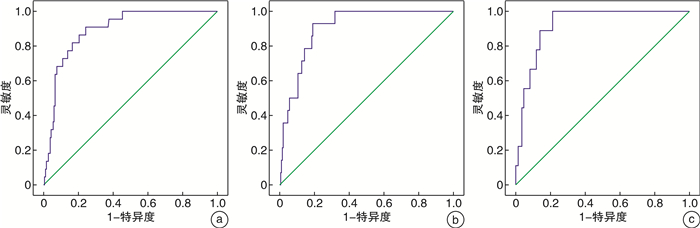
表 3 入院时血清CitH3预测持续性器官衰竭、胰腺坏死及院内死亡的临床价值
预测变量 AUC P 灵敏度/% 特异度/% 约登指数 截断值 95%CI 持续性器官衰竭 0.891 <0.001 90.9 75.7 0.666 158.30 0.835~0.948 胰腺坏死 0.903 <0.001 92.9 81.0 0.739 187.85 0.849~0.958 院内死亡 0.924 <0.001 99.8 78.9 0.789 184.20 0.873~0.974
下载: 导出CSV
-
[1] 李军祥, 陈誩, 唐文富. 急性胰腺炎中西医结合诊疗共识意见(2017年)[J]. 中国中西医结合消化杂志, 2017, 25(12): 901-909. https://www.cnki.com.cn/Article/CJFDTOTAL-ZXPW201712004.htm
[2] 吕农华, 何文华. 急性胰腺炎的内镜治疗[J]. 临床肝胆病杂志, 2020, 36(8): 1688-1690. doi: 10.3969/j.issn.1001-5256.2020.08.002
[3] Zhou H, Mei X, He X, et al. Severity stratification and prognostic prediction of patients with acute pancreatitis at early phase: A retrospective study[J]. Medicine(Baltimore), 2019, 98(16): e15275.
[4] 关小容, 付斌, 郑永先, 等. 血清瓜氨酸化组蛋白H3、沉默信号调节因子1检测在急诊脓毒症患者病情及预后评估中应用研究[J]. 创伤与急危重病医学, 2021, 9(4): 268-271, 276. doi: 10.16048/j.issn.2095-5561.2021.04.05
[5] Hu J, Kang H, Chen H, et al. Targeting neutrophil extracellular traps in severe acute pancreatitis treatment[J]. Therap Adv Gastroenterol, 2020, 13: 1756284820974913.
[6] Pan B, Li Y, Liu Y, et al. Circulating CitH3 Is a Reliable Diagnostic and Prognostic Biomarker of Septic Patients in Acute Pancreatitis[J]. Front Immunol, 2021, 12: 766391. doi: 10.3389/fimmu.2021.766391
[7] Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus[J]. Gut, 2013, 62(1): 102-111. doi: 10.1136/gutjnl-2012-302779
[8] Huh JH, Kim JW, Lee KJ. Vitamin D deficiency predicts severe acute pancreatitis[J]. United European Gastroenterol J, 2019, 7(1): 90-95. doi: 10.1177/2050640618811489
[9] 李涛, 费素娟. 实验室指标对急性胰腺炎发生器官衰竭的预测价值[J]. 中国中西医结合消化杂志, 2021, 29(3): 218-221. doi: 10.3969/j.issn.1671-038X.2021.03.13
[10] Kong W, He Y, Bao H, et al. Diagnostic Value of Neutrophil-Lymphocyte Ratio for Predicting the Severity of Acute Pancreatitis: A Meta-Analysis[J]. Dis Markers, 2020, 2020: 9731854.
[11] Silva-Vaz P, Abrantes AM, Castelo-Branco M, et al. Multifactorial Scores and Biomarkers of Prognosis of Acute Pancreatitis: Applications to Research and Practice[J]. Int J Mol Sci, 2020, 21(1): 338. doi: 10.3390/ijms21010338
[12] 梁华益, 杨复锵, 潘路娟, 等. 外泌体在急性胰腺炎发病机制、诊断及治疗中作用的研究进展[J]. 山东医药, 2021, 61(17): 95-97. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYY202117026.htm
[13] Dumnicka P, Maduzia D, Ceranowicz P, et al. The Interplay between Inflammation, Coagulation and Endothelial Injury in the Early Phase of Acute Pancreatitis: Clinical Implications[J]. Int J Mol Sci, 2017, 18(2): 354. doi: 10.3390/ijms18020354
[14] 尹凯祥, 亓玉琴, 咸会波, 等. BISAP评分联合中性粒细胞/淋巴细胞比值对急性胰腺炎病情的早期预测价值[J]. 中国急救医学, 2019, 39(6): 551-554. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJJY201906006.htm
[15] 刘江, 白杨, 阿孜古丽·阿不都热依木, 等. 中性粒细胞单核细胞乘积联合血肌酐诊断急性胰腺炎严重程度的价值[J]. 南方医科大学学报, 2017, 37(9): 1270-1273. https://www.cnki.com.cn/Article/CJFDTOTAL-DYJD201709024.htm
[16] Wan J, Ren Y, Yang X, et al. The Role of Neutrophils and Neutrophil Extracellular Traps in Acute Pancreatitis[J]. Front Cell Dev Biol, 2020, 8: 565758.
[17] 马雪妮, 许慧梅, 程龙, 等. 中性粒细胞外诱捕网与炎症性肠病关系的研究进展[J]. 中国免疫学杂志, 2021, 37(23): 2937-2941. https://www.cnki.com.cn/Article/CJFDTOTAL-ZMXZ202123020.htm
[18] 袁燕文, 陈孟君, 许哲, 等. 急性胰腺炎患者血清cf-DNA/NETs、MAP1-LC3、DPB表达水平及临床意义[J]. 分子诊断与治疗杂志, 2021, 13(7): 1055-1058, 1062. https://www.cnki.com.cn/Article/CJFDTOTAL-YXYQ202107010.htm
[19] 李慧, 邢广群. NETs刺激下慢性支气管炎大鼠血清ANCA产生机制探讨[J]. 中国免疫学杂志, 2017, 33(10): 1458-1463. https://www.cnki.com.cn/Article/CJFDTOTAL-ZMXZ201710004.htm
[20] Pan B, Alam HB, Chong W, et al. CitH3: a reliable blood biomarker for diagnosis and treatment of endotoxic shock[J]. Sci Rep, 2017, 7(1): 8972.
[21] Deng Q, Pan B, Alam HB, et al. Citrullinated Histone H3 as a Therapeutic Target for Endotoxic Shock in Mice[J]. Front Immunol, 2019, 10: 2957.
[22] Dąbrowska D, Jabłońska E, Garley M, et al. New Aspects of the Biology of Neutrophil Extracellular Traps[J]. Scand J Immunol, 2016, 84(6): 317-322.
-
图(3)
表(3)
计量
- 文章访问数: 844
- PDF下载数: 344
- 施引文献: 0