
Comparative study on clinical efficacy of indobufen and aspirin in acute mild ischemic stroke
-
摘要: 目的 对比吲哚布芬与阿司匹林治疗急性轻型缺血性脑卒中的临床疗效。方法 选取2021年1月—2021年9月期间住院治疗的急性轻型缺血性脑卒中患者60例,采用随机数字表法分为2组:观察组(n=30)与对照组(n=30)。2组均接受基础治疗,观察组口服吲哚布芬,对照组口服阿司匹林,前3周2组均联合氯吡格雷口服,3周后观察血小板聚集功能,90 d后观察2组患者的美国国立卫生院神经功能缺损(NIHSS)评分变化、Barthel指数(BI)变化及不良反应发生情况。结果 2组患者的基线特征具有可比性(P>0.05)。2组患者治疗前花生四烯酸(AA)诱导的血小板最大聚集率(MAR-AA)和二磷酸腺苷(ADP)诱导的血小板最大聚集率(MAR-ADP)具有可比性(P>0.05);治疗3周后均降低,差异有统计学意义(P< 0.05),2组治疗后比较差异无统计学意义(P>0.05)。治疗前2组NIHSS评分具有可比性(P>0.05);治疗3个月后均降低,差异有统计学意义(P< 0.05),治疗后2组NIHSS评分比较差异无统计学意义(P>0.05)。治疗前2组BI指数比较差异无统计学意义(P>0.05);治疗后,2组BI指数较用药前均升高,差异有统计学意义(P< 0.05),且2组间BI指数评分差异无统计学意义(P>0.05)。观察组发生不良反应情况较对照组低(3.33% vs. 23.33%,P< 0.05)。结论 2组药物方案抗血小板聚集效果相当,且均能改善急性轻型缺血性脑卒中患者的神经功能缺损、日常生活能力,但吲哚布芬不良反应发生率更低,安全性更高。吲哚布芬对急性轻型缺血性脑卒中的治疗作用与阿司匹林相当,且不良反应更小。
-
关键词:
- 吲哚布芬 /
- 阿司匹林 /
- 急性轻型缺血性脑卒中 /
- 疗效
Abstract: Objective To compare the clinical efficacy of indobufen and aspirin in the treatment of acute mild ischemic stroke.Methods Sixty patients with acute mild ischemic stroke hospitalized in the Department of Neurology of our hospital from January 2021 to September 2021 were selected and divided into 2 groups by random number table method: observation group(n=30) and control group(n=30), both groups received basic treatment, the observation group orally indocybufen, the control group orally aspirin, the first 3 weeks of both groups combined with clopidogrel, 3 weeks after observation of platelet aggregation function, 90 days after observation of NIH stroke scale(NIHSS), Barthe index(BI) changes, and the occurrence of adverse reactions in 2 groups.Results The baseline characteristics of the two groups were comparable(P>0.05). Before treatment, MAR-AA and MAR-ADP were comparable between 2 groups(P>0.05). There was significant difference before and after treatment(P< 0.05), but there was no significant difference between the two groups after treatment(P>0.05). NIHSS scores were comparable between 2 groups before treatment(P>0.05). There was significant difference before and after treatment(P< 0.05), while NIHSS score after treatment between the two groups had no statistical significance(P>0.05). BI index was comparable between 2 groups before treatment(P>0.05). After 3 months of treatment, BI index scores of patients in both groups increased(P< 0.05). There was no significant difference in BI index between the two groups after treatment(P>0.05). After treatment, there were fewer adverse reactions in the observation group than the control group(3.33% vs. 23.33%,P< 0.05).Conclusion The anti-platelet aggregation effect of the two groups of drug regimen is similar, and both can improve the neurological deficit and daily living ability of patients with acute mild ischemic stroke, but the incidence of adverse reactions of indocybufen is lower, and the safety is higher. In conclusion, indocybufen has the same therapeutic effect as aspirin in the treatment of acute mild ischemic stroke with fewer side effects.-
Key words:
- indobufen /
- aspirin /
- acute mild ischemic stroke /
- efficacy
-

-
表 1 2组患者基本资料的比较
例,X±S 基本资料 实验组(n=30) 对照组(n=30) P 性别 男 19 22 0.405 女 11 8 年龄/岁 60.57±7.68 62.70±6.98 0.682 高血压病史 有 12 19 0.070 无 18 11 高脂血症病史 有 4 3 0.688 无 26 27 糖尿病史 有 9 8 0.774 无 21 22 吸烟史 有 16 15 0.796 无 14 15 饮酒史 有 8 13 0.176 无 22 17  下载: 导出CSV
下载: 导出CSV
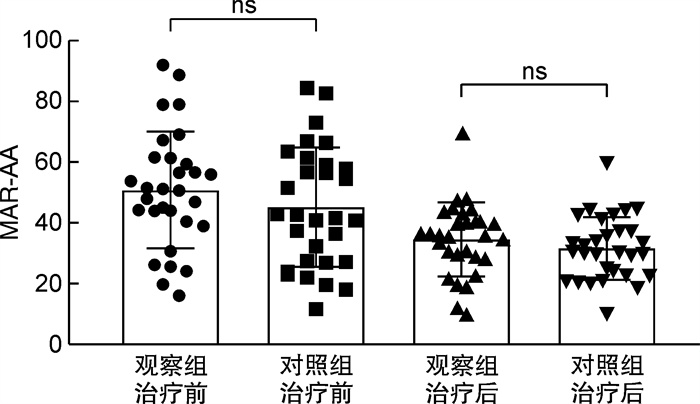
表 2 2组患者治疗前后MAR-AA的比较
%,X±S 组别 MAR-AA P 治疗前 治疗后 观察组 50.786 7±19.165 5 34.683 3±11.876 9 0.015 对照组 44.946 7±19.658 9 31.630 0±10.355 4 < 0.001 P 0.249 0.293
下载: 导出CSV
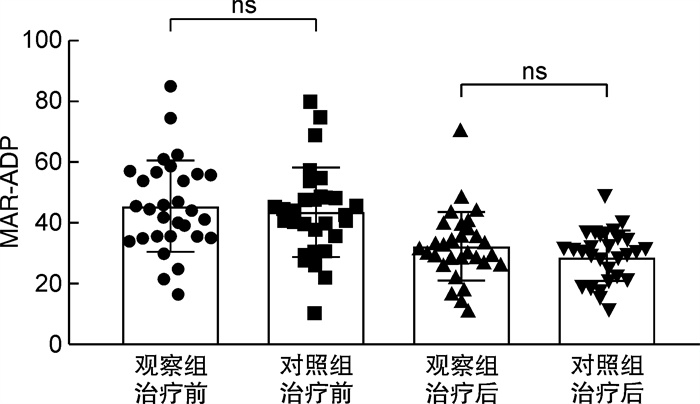
表 3 2组患者治疗前后MAR-ADP的比较
%,X±S 组别 MAR-ADP P 治疗前 治疗后 观察组 45.683 3±14.950 5 32.456 7±11.292 8 0.024 对照组 43.573 3±14.673 4 29.496 7±8.226 1 0.001 P 0.583 0.251
下载: 导出CSV
表 4 2组患者治疗前后NIHSS评分的比较
分,M(Q1,Q3) 组别 NIHSS评分 P 治疗前 治疗后 观察组 2.00(1.00,2.25) 1.00(1.00,1.00) < 0.001 对照组 2.00(1.00,2.00) 1.00(0.75,1.00) 0.001 P 0.873 0.692
下载: 导出CSV
表 5 2组患者治疗前后BI指数的比较
分,X±S 组别 BI指数 P 治疗前 治疗后 实验组 85.500 0±8.024 7 91.500 0±7.673 3 0.004 对照组 87.000 0±8.051 6 91.500 0±6.966 7 0.001 P 0.860 0.607
下载: 导出CSV
-
[1] Wang W, Jiang B, Sun H, et al. Prevalence, Incidence, and Mortality of Stroke in China Clinical Perspectctive: Results from a Nationwide Population-Based Survey of 480687 Adults[J]. Circulation, 2017, 135(8): 759. doi: 10.1161/CIRCULATIONAHA.116.025250
[2] Wang Z, Li J, Wang C, et al. Gender differences in 1-year clinical characteristics and outcomes after stroke: Results from the China National Stroke Registry[J]. PLoS One, 2013, 8(2): e56459. doi: 10.1371/journal.pone.0056459
[3] Wang YJ, Jing JJ, Meng X, et al. The Third China National Stroke Registry(CNSR-Ⅲ)for patients with acute ischaemic stroke or transient ischaemic attack: design, rationale and baseline patient characteristics[J]. Stroke Vasc Neurol, 2019, 4(3): 158-164. doi: 10.1136/svn-2019-000242
[4] 潘岳松. 氯吡格雷联合阿司匹林治疗对轻型卒中与短暂性脑缺血发作患者功能预后的影响: CHANCE与POINT试验联合分析[J]. 中国卒中杂志, 2021, 16(2): 157-162. https://www.cnki.com.cn/Article/CJFDTOTAL-ZUZH202102010.htm
[5] Visonà A, Davanzo S, Bruno R. Antiaggregant effect of indobufen(K3920) measured by the platelet aggregate filtration pressure test(PAFP)[J]. J Int Med Res, 1983, 11(1): 10-14. doi: 10.1177/030006058301100103
[6] De Caterina R, Giannessi D, Bernini W, et al. A prostacyclin-sparing effect of indobufen vs. aspirin[J]. Thromb Haemost, 1996, 75(3): 510-514. doi: 10.1055/s-0038-1650306
[7] 刘娟娟, 洪源源, 汪星辉, 等. 阿司匹林与硫酸氢氯吡格雷治疗脑梗死的效果和对心理状态的改善观察[J]. 心理月刊, 2021(13): 77-78. https://www.cnki.com.cn/Article/CJFDTOTAL-XLYK202113032.htm
[8] 吴燕子, 叶珊, 刘芳. 阿司匹林联合氯吡格雷治疗进展性脑卒中有效性和安全性的Meta分析[J]. 中国药房, 2020, 31(2): 227-233. https://www.cnki.com.cn/Article/CJFDTOTAL-ZGYA202002019.htm
[9] Moussouttas M, Papamitsakis NIH. Critique on the Use of Early Short-Term Dual Antiplatelet Therapy Following Minor Acute Cerebral Ischemic Events[J]. Cerebrovasc Dis, 2020, 49(3): 237-243. doi: 10.1159/000508026
[10] Lanas A, Polo-Tomás M, Casado-Arroyo R. The Aspirin cardiovascular/gastrointestinal risk calculator-a tool to aid clinicians in practice[J]. Alimentary Pharmacolo Therapeut, 2013, 37(7): 738-748. doi: 10.1111/apt.12240
[11] 马兰. 阿司匹林联合氯吡格雷治疗急性脑梗死的临床效果及不良反应发生情况分析[J]. 中国现代药物应用, 2021, 15(10): 164-166. https://www.cnki.com.cn/Article/CJFDTOTAL-ZWYY202110063.htm
[12] 张明辉, 张红卫, 高云, 等. 阿司匹林抗血小板治疗的药学研究及不良反应[J]. 中国实用医药, 2021, 16(26): 183-185. https://www.cnki.com.cn/Article/CJFDTOTAL-ZSSA202126074.htm
[13] Inzitari D. The italian guidelines for stroke prevention. The stroke prevention and educational awareness diffusion(SPREAD)colaboration[J]. Neurol Sci, 2000, 21(1): 5-12. doi: 10.1007/s100720070112
[14] 杨霞, 刘维, 陈恳, 等. 吲哚布芬片预防和治疗缺血性心脑血管病变有效性和安全性的Meta分析[J]. 中国临床药理学杂志, 2017, 33(4): 359-362. https://www.cnki.com.cn/Article/CJFDTOTAL-GLYZ201704019.htm
[15] Temporelli PL, Zito GB, Pedretti RF, et al. Nonsteroid anti-inflammatory drugs(NSAID)and risk of cardiovascular events. Literature review and clinical implications[J]. Monaldi Arch Chest Dis, 2014, 82(3): 165-170.
[16] Lee JY, Sung KC, Choi HI. Comparison of aspirin and indobufen in healthy volunteers[J]. Platelets, 2016, 27(2): 105-109.
[17] Balucani C, Levine SR, Khoury JC, et al. Acute Ischemic Stroke with Very Early Clinical Improvement: A National Institute of Neurological Disorders and Stroke Recombinant Tissue Plasminogen Activator Stroke Trials Exploratory Analysis[J]. J Stroke Cerebrovasc Dis, 2016, 25(4): 894-901. doi: 10.1016/j.jstrokecerebrovasdis.2015.10.028
[18] Li QX, ZhaLi QX, Zhao XJ, et al. Value of the Barthel scale in prognostic prediction for patients with cerebral infarction[J]. BMC Cardiovasc Disord, 2020, 20(1): 14. doi: 10.1186/s12872-019-01306-1
[19] 陈缙, 张海洋, 吴同果. 血小板聚集功能检测的临床应用[J]. 心脏杂志, 2015, 27(6): 732-735. https://www.cnki.com.cn/Article/CJFDTOTAL-XGNZ201506027.htm
[20] 杨琨, 孙佳凡. 吲哚布芬治疗急性脑梗死的临床疗效观察[J]. 中国医药, 2012, 7(2): 144-145.
[21] De CR, Giannessi D, Bernini W, et al. A prostacyclin-sparing effect of indobufen vs aspirin[J]. J Thromb Thrombolys, 1996, 75(3): 510-514.
[22] 刘想林, 王茹莹, 徐平. 阿司匹林与氯吡格雷对急性脑梗死患者血小板聚集率的影响比较[J]. 临床合理用药杂志, 2021, 14(19): 1-3. https://www.cnki.com.cn/Article/CJFDTOTAL-PLHY202119001.htm
[23] 邬义强. 吲哚布芬与拜阿司匹林联合氯吡格雷治疗急性冠脉综合征的临床比较[J]. 中外医学研究, 2020, 18(32): 40-42. https://www.cnki.com.cn/Article/CJFDTOTAL-YJZY202032016.htm
[24] 王阳, 姜玉龙, 杨位霞, 等. 阿司匹林联合硫酸氢氯吡格雷口服治疗脑梗死患者临床疗效及对神经功能缺损评分影响观察[J]. 山西医药杂志, 2021, 50(13): 2057-2060. https://www.cnki.com.cn/Article/CJFDTOTAL-SXYY202113015.htm
[25] Barillà F, Pulcinelli FM, Mangieri E, et al. Clopidogrel plus indobufen in acute coronary syndrome patients with hypersensitivity to aspirin undergoing percutaneous coronary intervention[J]. Platelets, 2013, 24(3): 183-188. doi: 10.3109/09537104.2012.686072
[26] Inzitari D. The italian guidelines for stroke prevention. The stroke prevention and educational awareness diffusion(SPREAD)colaboration[J]. Neurol Sci, 2000, 21(1): 5-12. doi: 10.1007/s100720070112
[27] Sugisaki N, Iwakiri R, Tsuruoka N, et al. A case-control study of the risk of upper gastrointestinal mucosal injuries in patients prescribed concurrent NSAIDs and antithrombotic drugs based on data from the Japanese national claims database of 13million accumulated patients[J]. J Gastroenterol, 2018, 53(12): 1253-1260. doi: 10.1007/s00535-018-1483-x
[28] 吴冰冰, 梅琼. 阿司匹林不良反应的国内文献分析[J]. 中国药师, 2008, 11(2): 224-225. doi: 10.3969/j.issn.1008-049X.2008.02.052
[29] 张成梅, 尹志圣, 武传涛, 等. 吲哚布芬对血小板聚集及血栓形成的影响[J]. 山东大学学报, 2010, 48(12): 37-41. https://www.cnki.com.cn/Article/CJFDTOTAL-SDYB201012010.htm
[30] 刘怡, 姜红菊. 吲哚布芬与阿司匹林治疗急性冠脉综合征的疗效比较[J]. 实用医药杂志, 2020, 37(7): 616-618. https://www.cnki.com.cn/Article/CJFDTOTAL-QEYY202007014.htm
-
图(2)
表(5)
计量
- 文章访问数: 1714
- PDF下载数: 1897
- 施引文献: 0