
Summary of experience in 18 cases of intestinal perforation caused by ingestion of single center jujube stones
-
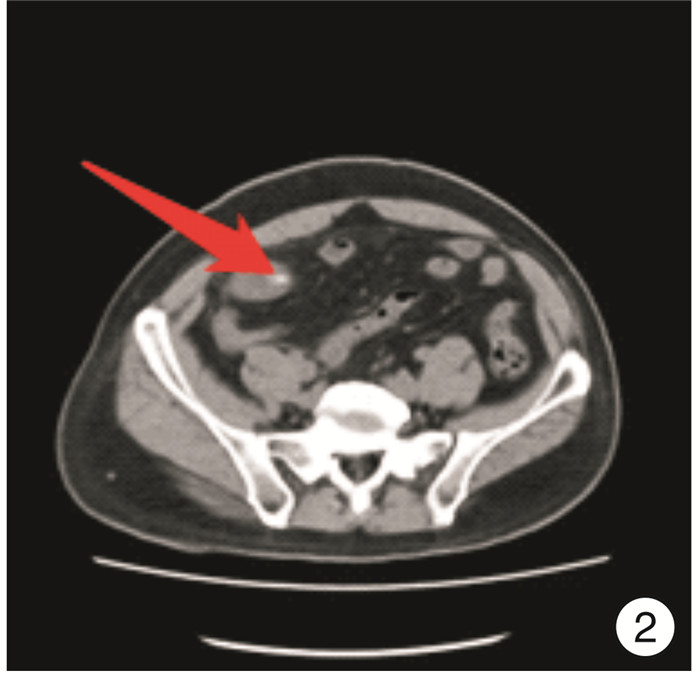
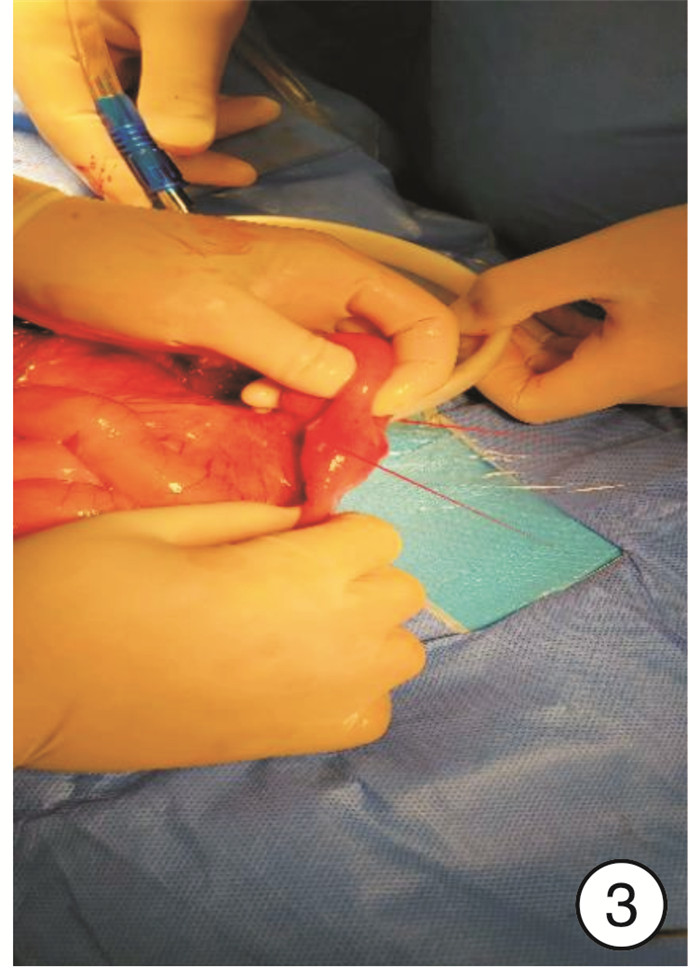
摘要: 目的 总结我院误食枣核导致小肠穿孔患者的诊治经验,为临床急腹症的诊疗提供临床经验,以便为该种少见急腹症的早期诊断和治疗提供参考。方法 回顾性收集2019年2月—2022年6月期间陕西省人民医院普外科和急诊外科收治的18例误食枣核致小肠穿孔患者行手术治疗的临床资料并对患者数据行总结分析。结果 18例患者中,男4例,女14例;平均年龄为62.3岁;10例患者有明确的术前误食枣核的病史;患者主要临床表现为腹痛,其中3例患者伴体温升高。8例患者行肠穿孔修补术,10例患者行肠切除+吻合术;3例患者在手术后入住重症监护室。18例患者的术后住院时间为3~27 d,平均为11.3 d。结论 老年患者为误食枣核的高危人群,术前CT及相关病史是误食枣核致小肠穿孔的重要诊治方法;患者保守治疗效果不佳,出现弥漫性腹膜炎、脓毒血症等严重并发症时,应及时手术。Abstract: Objective To summarize the diagnosis and the experience of patients with intestinal perforation caused by eating data pit by mistake in our hospital, and to provide clinical experience for the diagnosis and treatment of clinical acute abdomen, so as to provide reference for the early diagnosis and treatment of this rare acute abdomen.Methods From February 2019 to June 2022, a total of 18 patients who underwent surgical treatment due to intestinal perforation caused by wrongly eating data pit were collected and retrospectively analyzed.Results There were 4 males and 14 females, with an average age of 62.3 years. 10 patients had a clear history of wrongly eating data pit before surgery. And the main clinical manifestations were abdominal pain, and 3 of them were accompanied by elevated body temperature. 8 patients underwent intestinal perforation repair, 10 patients underwent intestinal excision and anastomosis, and 3 patients were admitted to the intensive care unit after surgery. The mean postoperative hospital stay for the 18 patients was 11.3 days(from 3 to 27 days).Conclusion Elderly patients are at high risk of ingestion of date pit. Preoperative CT and related medical history are important methods for the diagnosis and treatment of small bowel perforation caused by ingestion of date pit. Conservative treatment is not effective, and surgery should be performed in time when serious complications such as diffuse peritonitis and sepsis occur.
-
Key words:
- data pit /
- intestinal perforation /
- elderly /
- surgery
-

-
表 1 18例误食枣核致小肠穿孔患者资料
编号 性别 年龄/岁 临床表现 WBC/(×109/L) PCT/(ng/mL) 影像学表现 穿孔位置 手术方式 术中所见 排气排便时间/d 是否入住ICU 腹部平片 腹部CT 1 女 86 腹痛腹胀 4.02 — — — 距回盲部5 cm 肠穿孔修补术 腹腔积液 3 否 2 女 56 腹痛、恶心呕吐 13.32 — — 梭形高密度影 距回盲部110 cm 肠切除+吻合术 腹腔积液、脓苔 3 否 3 女 75 腹痛、恶心呕吐 10.73 — 未见异常 梭形高密度影 距回盲部1.5 cm 肠切除+吻合术 — 6 否 4 男 63 腹痛 11.19 1.14 — 梭形高密度影 距回盲部30 cm 肠穿孔修补术 腹腔积液 6 否 5 女 77 腹痛、发热 12.13 7.30 未见异常 腹腔游离气体、局部肠管扩张伴积气积液 — 肠穿孔修补术 腹腔积液、脓苔、局部肠管粘连 7 是 6 女 47 腹痛 6.81 0.59 — 梭形高密度影 距回盲部10 cm 肠穿孔修补术 腹腔积液、局部肠管粘连 3 否 7 男 58 腹痛 12.32 0.62 肠气增多、局部气液平 梭形高密度影、腹腔游离气体 距回盲部60 cm 肠切除+吻合术 腹腔积液、局部肠管粘连 5 否 8 女 62 腹痛腹胀、恶心呕吐 7.96 14.87 — 梭形高密度影、腹腔游离气体 距回盲部100 cm 肠切除+吻合术 腹腔积液、局部肠管粘连 2 是 9 男 62 腹痛、恶心呕吐 8.55 4.27 — 梭形高密度影、腹腔游离气体 距回盲部4 cm 肠切除+吻合术 脓苔、局部肠管粘连 2 否 10 女 19 腹痛、恶心呕吐 15.55 0.87 肠气增多、局部气液平 梭形高密度影、局部肠管扩张伴积气积液 距回盲部1.5 cm 肠切除+吻合术 — 2 否 11 女 63 腹痛、恶心发热 6.88 3.79 — 梭形高密度影 距回盲部200 cm 肠切除+吻合术 — 3 否 12 女 68 腹痛、恶心呕吐 10.19 9.28 — 梭形高密度影、腹腔游离气体 距回部20 cm 肠穿孔修补术 腹腔积液 — 是 13 女 69 腹痛 7.27 4.40 — 梭形高密度影 距回盲部100 cm 肠穿孔修补术 腹腔积液、脓苔、局部肠管粘连 2 否 14 女 59 腹痛腹胀、恶心呕吐 14.67 3.64 — 梭形高密度影、局部肠管扩张伴积气积液 十二指肠球部 肠穿孔修补术 腹腔积液、脓苔 — 否 15 女 51 腹痛 11.50 — — — 距回盲部40 cm 肠切除+吻合术 腹腔积液、脓苔 — 否 16 男 76 腹痛 10.40 5.03 — 梭形高密度影、局部肠管扩张伴积气积液 距回盲部120 cm 肠切除+吻合术 腹腔积液、脓苔 — 否 17 女 68 腹痛 13.91 — — 梭形高密度影、腹腔游离气体 距回盲部65 cm 肠穿孔修补术 — 5 否 18 女 62 腹痛、发热 7.22 21.82 — 梭形高密度影、局部肠管扩张伴积气积液 距回盲部30 cm 肠切除+吻合术 — 5 否  下载: 导出CSV
下载: 导出CSV
-
[1] Li F, Zhou X, Wang B, et al. Intestinal perforation secondary to pits of jujube ingestion: A single-center experience with 18 cases[J]. World J Surgery, 2019, 43(5): 1198-206. doi: 10.1007/s00268-018-04902-y
[2] Ho JPK, Jameson C. Small bowel perforation from foreign body ingestion[J]. ANZ J Surg, 2019, 89(10): 1336-1337. doi: 10.1111/ans.14715
[3] Villanueva Campos AM, Martinez Rodriguez C, Tardaguila FG, et al. Gastrointestinal perforation caused by ingested fish bone. Computed tomography findings in 58 patients[J]. Radiologia, 2020, 62(5): 384-391. doi: 10.1016/j.rx.2020.01.003
[4] Ross JT, Matthay MA, Harris HW. Secondary peritonitis: principles of diagnosis and intervention[J]. BMJ, 2018, 361: k1407.
[5] 寇玉彬, 盛春, 陆运松. 急诊老年患者消化道异物致胃肠道穿孔的临床特点及诊治[J]. 临床急诊杂志, 2021, 22(11): 776-778. doi: 10.13201/j.issn.1009-5918.2021.11.014
[6] Langell JT, Mulvihill SJ. Gastrointestinal perforation and the acute abdomen[J]. Medical Clin North Am, 2008, 92(3): 599-625. doi: 10.1016/j.mcna.2007.12.004
[7] Merayo-Álvarez M, Fernández-Martinez D, Gonzales-Stuva J, et al. Perforation of Meckel's diverticulum by a foreign body[J]. Rev Gastroenterol Mex(Engl Ed), 2019, 84(1): 112-114.
[8] 阮华兵, 王东. 中性粒细胞/淋巴细胞比值与血小板/淋巴细胞比值在上消化道溃疡穿孔中的鉴别诊断价值[J]. 临床急诊杂志, 2020, 21(2): 147-152. doi: 10.13201/j.issn.1009-5918.2020.02.010
[9] Kroon HM, Mullen D. Ingested foreign body causing a silent perforation of the bowel[J]. BMJ Case Reports, 2021, 14(1): e240879. doi: 10.1136/bcr-2020-240879
[10] Lin N, Lin L, Wu W, et al. Successful diagnosis and treatment of ingested wooden toothpicks: Two case reports[J]. Medicine, 2018, 97(5): e9710. doi: 10.1097/MD.0000000000009710
[11] 赵益林, 陈军, 许启仲. 64排螺旋CT及其后处理技术在老年人食管异物诊断中的价值[J]. 临床急诊杂志, 2015, 16(4): 290-292. doi: 10.13201/j.issn.1009-5918.2015.04.014
[12] Wu CW, Chiu YW. Unintentional fish bone ingestion causing perforation of small intestine[J]. Int Emerg Med, 2021, 16(5): 1371-1372. doi: 10.1007/s11739-020-02519-5
[13] Chia M, Chai VW, Modak P. Delayed small bowel perforation after accidental bread clip ingestion[J]. Anz J Surg, 2022, 92(10): 2747-2748. doi: 10.1111/ans.17562
[14] Shi X, Shan Y, Yu E, et al. Lower rate of colonoscopic perforation: 110 785 patients of colonoscopy performed by colorectal surgeons in a large teaching hospital in China[J]. Surg Endoscopy, 2014, 28(8): 2309-2316. doi: 10.1007/s00464-014-3458-1
[15] Taguchi T, Kitagawa H. Fish bone perforation[J]. N Engl J Med, 2019, 381(8): 762. doi: 10.1056/NEJMicm1900442
[16] Kathayat LB, Chalise A, Maharjan JS, et al. Intestinal perforation with ingestion of blunt foreign bodies: A case report[J]. JNMA, 2022, 60(253): 817-820.
[17] Ward MA, Tews MC. Small bowel perforation secondary to fish bone ingestion managed non-operatively[J]. J Emerg Med, 2012, 43(5): 295-298. doi: 10.1016/j.jemermed.2010.05.039
[18] Ihoriya H, Ichiba T. Ingestion of eggshell resulting in small bowel perforation[J]. Anz J Surgery, 2021, 91(1-2): E84-E85.
[19] Wu C, Khan N, Yuan X, et al. Duodenal perforation caused by iron bar[J]. Am J Gastroenterol, 2018, 113(10): 1429. doi: 10.1038/s41395-018-0263-9
[20] Wang R, He J, Chen Z, et al. Migration of fish bones into abdominal para-aortic tissue from the duodenum after leading to duodenal perforation: a case report[J]. BMC Gastroenterol, 2021, 21(1): 82. doi: 10.1186/s12876-021-01662-3
[21] John M, Stern G, Cameron F, et al. Piercing issue: a 10-year single-centre experience of magnet ingestion in children[J]. Arch Dis Child, 2021, 106(12): 1243-1244. doi: 10.1136/archdischild-2021-321848
[22] Demir MK, Turanoglur H, Yilmaz S. Fishbone perforation of the terminal ileum mimicking acute appendicitis[J]. Br J Hosp Med, 2022, 83(12): 1.
[23] Li XL, Zhang QM, Lu SY, et al. Clinical report and analysis of 24 cases of multiple magnetic beads foreign body in gastrointestinal tract of children[J]. Turkish J Gastroenterol, 2020, 31(11): 819-824. doi: 10.5152/tjg.2020.19600
[24] Morais R, Marques M, Macedo G. Endoscopic treatment of a foreign body-associated colonic perforation[J]. Int J Colorectal Dis, 2020, 35(1): 165-167. doi: 10.1007/s00384-019-03465-1
[25] Yao YY, Feng L. A patient with acute abdominal pain caused by an unnoticed swallowed toothpick misdiagnosed as acute appendicitis[J]. Arch Iranian Med, 2022, 25(4): 274-276. doi: 10.34172/aim.2022.44
-
图(4)
表(1)
计量
- 文章访问数: 629
- PDF下载数: 633
- 施引文献: 0