
Correlation between factor ⅩⅢ level and risk of hemorrhagic transformation in acute stroke patients after thrombolytic therapy
-
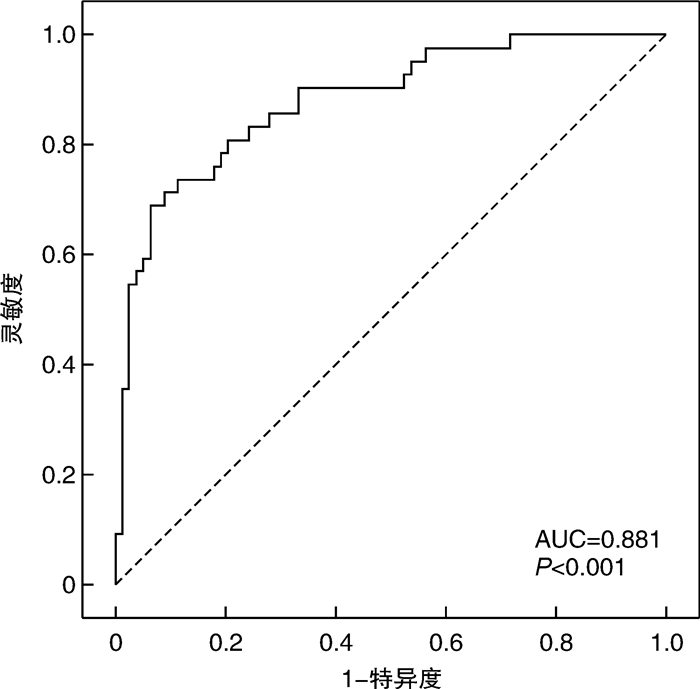
摘要: 目的 探讨急性缺血性脑卒中(AIS)患者静脉溶栓前凝血因子ⅩⅢ(FⅩⅢ)水平与溶栓后出血转化(HAT)风险的相关性,分析影响溶栓后HAT的危险因素。方法 纳入2020年3月—2021年8月万宁市人民医院卒中中心收治的行阿替普酶静脉溶栓治疗的AIS患者120例,收集所有患者临床和实验室资料,采用ELISA法检测患者溶栓前凝血指标和FⅩⅢ水平;根据患者溶栓后是否出现出HAT分为HAT组和非HAT组,比较2组患者的临床资料,采用logistic回归模型分析影响AIS患者溶栓后HAT风险的危险因素,绘制ROC曲线分析溶栓前FⅩⅢ水平在早期预测AIS出现HAT的诊断价值。结果 120例患者接受阿替普酶静脉溶栓后共出现42例HAT;对比2组临床资料显示,HAT组患者年龄≥80岁比例、梗死灶面积、NIHSS评分及血糖水平、FⅩⅢ水平与非HAT组比较,差异有统计学意义(P < 0.05);多因素logistic回归分析显示,年龄≥80岁(OR=9.465,P=0.004)、NIHSS评分越高(OR=1.577,P=0.010)、血糖水平(OR=1.314,P=0.007)是AIS患者溶栓后出现HAT的独立危险因素;FⅩⅢ水平(OR=0.836,P < 0.001)是AIS患者溶栓后出现HAT的独立保护因素。ROC曲线分析显示,溶栓前FⅩⅢ水平在早期预警AIS患者溶栓后出现HAT的AUC为0.881,灵敏度为69.05%,特异度为93.59%,截点值为66.215%。结论 AIS患者溶栓前FⅩⅢ水平可能是早期预警HAT的标志物,并具有较好的预测效能。Abstract: Objective To explore the correlation between the level of coagulation factor ⅩⅢ (FⅩⅢ) before intravenous thrombolysis and the hemorrhagic transformation(HAT) after thrombolysis in patients with acute ischemic stroke(AIS), and analyze the risk factors affecting HAT after thrombolysis.Methods From March 2020 to August 2021, 120 patients with AIS who were treated with rt-PA intravenous thrombolysis in our hospital's stroke center were enrolled. The clinical and laboratory data of all patients were collected, and ELISA was used to detect the coagulation of patients before thrombolysis. The patients were divided into HAT group and non-HAT group according to whether HAT occurred after thrombolysis. The clinical data of the two groups of patients were compared, and the logistic regression model was used to analyze the risk factors affecting the risk of HAT in patients with AIS after thrombolysis, and the ROC curve was used to analyze the diagnostic value of FⅩⅢ level before thrombolysis in early prediction of HAT.Results Among the 120 patients who received rt-PA intravenous thrombolysis, 42 cases of HAT occurred. There were significant differences in the proportion of patients age ≥80 years, infarct size, NIHSS score, blood glucose level and FⅩⅢ level in the HAT group compared with the non-HAT group (P < 0.05). Multivariate logistic regression analysis showed that age ≥80 years(OR=9.465, P=0.004), NIHSS score(OR=1.577, P=0.010), blood glucose level(OR=1.314, P=0.007) were the independent risk factors for HAT in AIS patients after thrombolysis; FⅩⅢ level(OR=0.836, P < 0.001) was an independent protective factor for HAT after thrombolysis in AIS patients. ROC curve analysis showed that the AUC of FⅩⅢ level before thrombolysis in early warning AIS patients with HAT after thrombolysis was 0.881, the sensitivity was 69.05%, the specificity was 93.59%, and the cut-off value was 66.215%.Conclusion The level of factor ⅩⅢ before thrombolysis in patients with AIS may be a marker for early warning of HAT, and it has good predictive performance.
-

-
表 1 2组患者临床资料比较
例,X±S 临床资料 HAT组
(n=42)非HAT组
(n=78)t/χ2/F P 性别 0.064 0.801 男 32 61 女 10 17 年龄/岁 4.575 0.032 ≥80 29 38 < 80 13 40 基础疾病 高血压病 33 63 0.082 0.774 糖尿病 6 10 0.051 0.822 冠心病 10 19 0.006 0.937 NIHSS评分/分 9.11±2.35 7.42± 1.98 4.173 < 0.001 GCS评分/分 10.45±2.56 10.28± 2.79 0.327 0.744 既往史 吸烟史 10 18 0.008 0.928 饮酒史 21 40 0.018 0.893 罪犯血管 0.132 0.716 大脑中动脉 23 40 穿支动脉 19 38 梗死灶面积 4.067 0.044 大面积脑梗死 28 37 腔隙性脑梗死 14 41 CT征象 致密动脉征 3 6 0.012 0.913 白质疏松 5 9 0.003 0.952 侧支循环 4 8 0.016 0.898  下载: 导出CSV
下载: 导出CSV
表 2 2组患者实验室指标比较
X±S 实验室指标 HAT组(n=42) 非HAT组(n=78) t P 生化指标 总胆固醇/(mmol·L-1) 4.49±1.51 4.53±1.26 0.155 0.877 低密度脂蛋白/(mmol·L-1) 2.23±0.38 2.25±0.44 0.249 0.804 高密度脂蛋白/(mmol·L-1) 0.85±0.23 0.82±0.19 0.765 0.446 甘油三酯/(mmol·L-1) 1.33±0.27 1.36±0.31 0.528 0.598 随机血糖/(mmol·L-1) 10.23±3.74 7.25±2.88 4.858 < 0.001 凝血指标 PLT/(×109·L-1) 220.45±52.38 213.41±48.92 0.733 0.465 PT/s 13.52±1.22 13.57±1.46 0.189 0.850 APTT/s 38.64±2.87 38.89±3.22 0.421 0.675 FIB/(g·L-1) 4.12±0.99 4.07±1.02 0.259 0.796 DD/(μg·L-1) 0.89±0.12 0.86±0.11 1.380 0.170 FⅩⅢ/% 60.23±9.72 77.59±10.36 9.465 < 0.001
下载: 导出CSV
表 3 赋值表
相关指标 变量 赋值 年龄 X1 ≥80岁=1, < 80岁=0 梗死灶面积 X2 大面积梗死=1,腔隙性梗死=0 NIHSS评分 X3 连续变量 随机血糖 X4 连续变量 FⅩⅢ X5 连续变量 HAT Y 是=1,否=0
下载: 导出CSV
表 4 影响AIS患者溶栓后发生HAT的logistic回归分析
相关指标 β 标准误 Wald P OR 95%CI 下限 上限 年龄≥80岁 2.248 0.774 8.427 0.004 9.465 2.075 43.168 大面积脑梗死 0.017 0.767 < 0.001 0.982 1.017 0.226 4.573 NIHSS评分 0.456 0.178 6.561 0.010 1.577 1.113 2.235 血糖 0.273 0.101 7.259 0.007 1.314 1.077 1.603 FⅩⅢ -0.179 0.036 24.415 < 0.001 0.836 0.779 0.897 常量 -15.779 6357.627 < 0.001 0.998 < 0.001
下载: 导出CSV
-
[1] 蒋陈晓, 仝瀚文, 王军, 等. 急性缺血性脑卒中阿替普酶静脉溶栓后症状性脑出血的临床分析[J]. 实用药物与临床, 2018, 21(6): 641-646. https://www.cnki.com.cn/Article/CJFDTOTAL-LYLC201806009.htm
[2] 孔晗鑫, 应豪. 影像学预测急性缺血性脑卒中出血转化的研究进展[J]. 实用放射学杂志, 2021, 37(4): 679-682. doi: 10.3969/j.issn.1002-1671.2021.04.041
[3] Osaki T, Souri M, Ichinose A. Important roles of the human leukocyte antigen class Ⅰ and Ⅱ molecules and their associated genes in the autoimmune coagulation factor ⅩⅢ deficiency via whole-exome sequencing analysis[J]. PLoS One, 2021, 16(9): e0257322. doi: 10.1371/journal.pone.0257322
[4] Zhang LJ, Zhang C, Luo Y, et al. Predictive value of coagulation factor ⅩⅢ on bleeding risk in ischemic stroke patients treated with intravenous thrombolysis[J]. Ann Palliat Med, 2021, 10(7): 7579-7586. doi: 10.21037/apm-21-1174
[5] 徐佩佩, 丁冰洁, 李梦娟, 等. 遗传性凝血因子ⅩⅢ缺乏症三例并文献复习[J]. 中华血液学杂志, 2021, 42(3): 256-258. https://www.cnki.com.cn/Article/CJFDTOTAL-LCJY202207019.htm
[6] 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004
[7] 王彬. 溶栓治疗急性缺血性脑卒中患者发生出血性转化的危险因素探讨[J]. 神经损伤与功能重建, 2019, 14(11): 568-570. https://www.cnki.com.cn/Article/CJFDTOTAL-GWKF201911009.htm
[8] Joksic I, Mikovic Z, Filimonovic D, et al. Combined presence of coagulation factor ⅩⅢ V34 L and plasminogen activator inhibitor 14G/5G gene polymorphisms significantly contribute to recurrent pregnancy loss in Serbian population[J]. J Med Biochem, 2020, 39(2): 199-207.
[9] 王艳芝, 谭榜云, 李琳, 等. 急性白血病患者化疗后骨髓抑制期血浆凝血因子ⅩⅢ水平及其对出血事件的影响[J]. 中华血液学杂志, 2020, 41(1): 59-63.
[10] Cai RM, Li Y, Wang WY, et al. A novel Cys328-terminator mutant implicated in severe coagulation factor ⅩⅢ deficiency: a case report[J]. BMC Med Genet, 2020, 21(1): 175. doi: 10.1186/s12881-020-01111-0
[11] 刘春梅, 周俊山, 施洪超, 等. 阿替普酶静脉溶栓治疗急性缺血性脑卒中后出血性转化的影响因素分析[J]. 中国神经免疫学和神经病学杂志, 2018, 25(3): 188-192. doi: 10.3969/j.issn.1006-2963.2018.03.008
[12] 张景忠, 齐英杰, 陈宇, 等. 急性缺血性脑卒中局部VLCBV与DWI及ADC在预测出血转化中的对比研究[J]. 卒中与神经疾病, 2019, 26(2): 165-168, 177. doi: 10.3969/j.issn.1007-0478.2019.02.008
[13] Schroeder V. Laboratory assessment of coagulation factor ⅩⅢ[J]. Hamostaseologie, 2020, 40(4): 467-471. doi: 10.1055/a-1181-0327
[14] Chan KYT, Yong ASM, Wang X, et al. The adhesion of clots in wounds contributes to hemostasis and can be enhanced by coagulation factor ⅩⅢ[J]. Sci Rep, 2020, 10(1): 20116.
[15] Hamedani NS, Biswas A, Rudan O, et al. Functional and structural characterization of nucleic acid ligands that bind to activated coagulation factor ⅩⅢ[J]. J Clin Med, 2021, 10(4): 677.
[16] 沈烨琪, 徐良额, 张圣, 等. 血清D-二聚体在急性缺血性脑卒中静脉溶栓出血转化及预后预测中的价值研究[J]. 浙江医学, 2020, 42(10): 1038-1042, 1047. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJYE202010015.htm
[17] Hur WS, Juang LJ, Mazinani N, et al. Post-translational modifications of platelet-derived amyloid precursor protein by coagulation factor ⅩⅢ-A[J]. Biochemistry, 2020, 59(46): 4449-4455.
[18] Ichinose A, Osaki T, Souri M. Pathological coagulation parameters in as many as 54 patients with autoimmune acquired factor ⅩⅢ deficiency due to anti-factor ⅩⅢ autoantibodies[J]. Haemophilia, 2021, 27(3): 454-462.
[19] Bronić A, Ferenčak G, Bernat R, et al. Association of fibrinogen and plasmin inhibitor, but not coagulation factor ⅩⅢ gene polymorphisms with coronary artery disease[J]. J Med Biochem, 2021, 40(2): 138-149.
[20] Vasilyeva AD, Yurina LV, Bugrova AE, et al. The nature of resistance of the coagulation factor ⅩⅢ structure to hypochlorite-induced oxidation[J]. Dokl Biochem Biophys, 2020, 495(1): 276-281.
-
图(1)
表(4)
计量
- 文章访问数: 494
- PDF下载数: 191
- 施引文献: 0